ACBS Strategic Plan: current strategic planning priorities/initiatives
ACBS Strategic Plan: current strategic planning priorities/initiatives
Strategic Planning Meeting
The ACBS Board strategic planning meeting was held and based off of ACBS member focus group data, and one on one interviews, a picture of the current state of the organization came into focus. The Board considered the arguments for what to keep and what to change within the organization. While we have much to be proud of as a community, the Board felt that the following four areas are priorities for change, so that we better execute our mission.
While this is still in the early stages, we wanted to share the four main strategic imperatives that were developed as a part of this meeting.

1. Expanding and improving our digital presence - The goal is for an improved and expanded digital platform and increased professional and public awareness and to become industry leaders in our science and dissemination. Carmine DiChiara - Lead; Tiffany Rochester - Champion
 2. Centering Science - Our goal is to make our support for science and research a more featured part of our work by doing more to support a robust worldwide research community within ACBS. Louise McHugh - Lead; Jonathan Bricker - Champion
2. Centering Science - Our goal is to make our support for science and research a more featured part of our work by doing more to support a robust worldwide research community within ACBS. Louise McHugh - Lead; Jonathan Bricker - Champion
 3. Creating a culture of empowerment and productivity - The goal is to help to make our Board, Committees, and Components more efficient and productive with clear goals and tasks and frequent communication. Jessica Borushok - Lead; Laura Silberstein-Tirch - Champion
3. Creating a culture of empowerment and productivity - The goal is to help to make our Board, Committees, and Components more efficient and productive with clear goals and tasks and frequent communication. Jessica Borushok - Lead; Laura Silberstein-Tirch - Champion
 4. Building a culture of competency to support effective dissemination in ACBS - Our goal is to support the ACBS community in developing and refining the science guiding best practices in training, competency measurement, application and dissemination of CBS. Robyn Walser - Lead; Nanni Presti - Champion
4. Building a culture of competency to support effective dissemination in ACBS - Our goal is to support the ACBS community in developing and refining the science guiding best practices in training, competency measurement, application and dissemination of CBS. Robyn Walser - Lead; Nanni Presti - Champion
Progress Update
- Sept. 2019 - Leads complete online Project Management Training
- Sept.-Oct. 2019 - Leads build core team
- Oct. 2019 - Leads hold first meeting with core teams
- Nov. 2019 - Outreach to Committees to collect relevant suggestions for the pillars
- Dec. 2019 - Core teams submit sketch outlines of their primary projects
- Jan. 2020 - Board members review the initial sketch outlines and provide feedback. Projects that most closely align with goals and with the best chance for success are selected for further development. All four teams are making good progress and moving forward with their work (adding a high level of detail to their initial sketches)
- February-August 2020 - Teams further develop their projects to add the high level of detail needed for the implementation phase (delays due to COVID-19)
- September-November 2020 - Teams submit final detailed plans for their primary projects
- November 2020 - Board appoints new lead for the Digital Pillar
- October-December 2020 - Board members review the detailed plans developed by each core team. Projects that most closely align with goals and with the best chance for success are selected to move forward
- November 2020 - Creating a Culture of Empowerment and Productivity Pillar has their primary projects approved and move on to planning stage (creating processes, procedures, templates, etc.)
- February 2021 - Centering Science Pillar is approved for 3 major projects and moves on to the planning stage
- February 2021 - Board looks to recruit new lead for the Digital Pillar
- April 2021 - Open call for Digital Pillar Lead. The Centering Science Pillar opens the application for the Early Career Mentee Program
- June 2021 - The Centering Science Pillar announces the CBS Superlab and the Contextual Behavioral Scientist-Practitioner Network at the 2021 Virtual Conference
- September 2021 - The first CBS Superlab session is held
- October 2021 - The Centering Science Pillar opens the application for the Interdisciplinary Science Capacity Building Seed Grant
- December 2021 - The Competency Pillar discussed a priority list for their primary projects with the Board, and are moving on to writing up their research to-date and additional planning
- August 2022 - The Inclusive Science Grant developed by the Centering Science Pillar opens as an additional ACBS Research Development Grant
- October 2022 - The Competency and Dissemination Working Group (Competency Pillar) creates a webpage of information and member resources
- February 2023 - The current and future Science Pillar projects will be managed under an ongoing Scientific Strategic Council (approved by the ACBS Board on February 1)
- May 2023 - An open call was sent out to membership to gather volunteers for the Scientific Strategic Council
- June 2023 - A new award opportunity for Chapters & SIGs was announced
- July 2023 - A chair and committee members for the Scientific Strategic Council were announced. The Competency Pillar presented some of their findings at the ACBS World Conference.

More detail about the Strategic Pillars
More detail about the Strategic PillarsAttached you can find more detail about the process and our strategic pillars.
Competency and Dissemination Working Group Homepage
Competency and Dissemination Working Group HomepageThe Working group for the Competency and Dissemination Strategic PIllar has been actively working to achieve the strategic goals established by the ACBS Board. This website is an ongoing effort to organize information relevant to issues of competency and dissemination of practices that fall under the umbrella of Contextual Behavioral Science.
What has the working group been doing?
Guided by this aim from the ACBS Board's call to action: “We envision a scientific community in which members of ACBS could find evidence informed guidelines on how to learn, how to apply, and how to measure their skill development over time,” the working group has
● Held bi-weekly and/or monthly meetings to determine the process and content of the information needed to create a thorough report for the ACBS Board.
● Reviewed definitions of competency and explored how to write about competency in ways that are consistent with the principles of CBS.
● Conducted an extensive literature review to assess the current published status of competency training in CBS approaches.
● Hosted two panels at the ACBS World Conference in 2022. One panel shared the results of the competency literature review. The other panel explored international issues in competency and dissemination.
● Hosted a panel at the ACBS World Conference in 2023 discussing the strengths, challenges, and future directions of competency assessment in contextual behavioral science approaches.
How is competency defined?
Competencies describe the behaviors to be displayed by all members of a community applying specified interventions with specified populations.
Competencies are complex and dynamically interactive clusters of behaviors that enable a person to execute a professional activity with a myriad of potential outcomes (Marrelli, 1998). These clusters may include:
● integrated knowledge of concepts and procedures;
● skills and abilities;
● behaviors and strategies;
● attitudes, beliefs, and values;
● dispositions and personal characteristics;
● self-perceptions; and
● motivations (Mentkowski, 2000)
Elements of Competencies involve the whole person and are:
● transmittable/teachable (relevant to effective dissemination)
● observable (behaviorally stated)
● measurable (based on assessment: exams or skills practice demonstration)
● containable (not so ambiguous as to be never-ending in nature)
● practical (implementable, applicable to a specific area)
● verifiable/linked to external validity
● parsimonious
● criterion referenced rather than norm referenced
● derived by experts
● interpersonal behaviors that support the therapeutic alliance (the behaviors need to be specified, reliable, trainable, etc.)
● flexible and transferable across settings
Competencies also need to be continually reevaluated and redefined as commensurate with new research findings. Supervision, training, and consultation are essential to this process. Supervision provides the context for competence to be developed, providing the essential tools to achieve ongoing development (initiating learning and ongoing skill uptake), performance monitoring, perspective-taking, and evaluating “meta-competence” - the ability to assess what one knows and what one doesn’t know. Meta-competence (perspective taking) helps fulfill the professional responsibility to pursue and support competence throughout one’s career.
Competency and Dissemination panels from the World Conference
- International Perspectives on CBS Competency and Dissemination - Panel presented by Sean Wright, Carmen Luciano, Zhuohong Zhu, Amanda Muñoz-Martinez, Steven Hayes, Hannah Bockarie (June 2022)
- Putting the task force report into action - Panel presented by Maria Karekla, Rhonda Merwin, Steven Hayes, Louise McHugh, Kenneth Fung (June 2022)
- Report from the ACBS Strategic Pillar for Competency and Dissemination - Panel presented by Raul Manzione, Alycia Zink, Sean Wright, Giovambattista Presti, Robyn Walser (June 2022)
- CBS Competencies: The good, the bad, and the need - Panel presented by Steve Hayes, Russell Kolts, Raul Manzione, Robyn Walser, and Sean Wright (July 2023)
Competency measures for CBS-informed approaches
Choose below
Compassion-Focused Therapy (CFT) - Competencies
Compassion-Focused Therapy (CFT) - CompetenciesOverview
Competencies for Compassion-Focused Therapy (CFT) have been established but have not been evaluated in research to date. Liddell, Allan, and Goss (2017) used a Delphi approach, recruiting 12 CFT experts to identify “the CFT competency framework (CFT-CF)”. This framework comprised six areas of competence: creating safeness, meta-skills, non-phase-specific skills, phase-specific skills, knowledge and understanding, and use of supervision. 25 primary competencies were identified within these areas.
Gilbert and Wood created an unpublished scale called the CFT Therapy Assessment Guide, a 45- item scale assessing “microskills, formulation skills, skills in explaining CFT, and contracting” (Horwood et al., 2020).
To build a more formal competency measure that included behavioral anchors, Horwood et al. (2020) used a Delphi approach and developed a CFT therapist competence rating scale (CFT-TCRS). The CFT-TCRS consists of 14 CFT unique competencies and 9 CFT microskills.
The CFT specific competencies include: psychoeducation, recognising motives and emotions, actively working with the three systems, understanding the relationship between three systems, compassionate mind training, building motivation, building courage, cultivating and tolerating positive feelings in the drive system, functional analysis, fears/blocks/resistances, unconscious emotions and processes, formulation, and multiple selves.
The CFT microskills include: non-verbal communication to build rapport, non-verbal communication and motivational/emotional systems, verbal communication, pacing, Socratic questioning, paraphrasing and summaries, agenda setting, validation and normalization, and mentalization.
Materials/Assessments/Work Products
CFT competency framework (CFT-CF)(Liddell, Allan, & Goss, 2017)
CFT therapist competence rating scale (CFT-TCRS) (Horwood et al., 2020)
Bell, Hickey, and Bennett-Levy (2022) described the benefits of self-practice/self-reflection (SP/SR) training specifically for CFT therapists. There is a SP/SR book for CFT therapists (Kolts et al., 2018). Bell, Dixon, and Kolts (2017) reported the qualitative results of a 4-week SP/SR approach for CFT trainees to develop a compassionate internal supervisor.
Additional guidance for therapists has been published in multiple books (Gilbert & Simos, 2022; Kolts, 2016).
Additionally, some CFT experts have been publishing on the benefit of self-practice/self-reflection as a means to develop competence in CBT more generally (Thwaites et al., 2014;2015).
References
Bell, T., Dixon, A., & Kolts, R. (2017). Developing a compassionate internal supervisor: Compassion‐focused therapy for trainee therapists. Clinical psychology & psychotherapy, 24(3), 632-648.
Bell, T., Hickey, T., & Bennett-Levy, J. (2022). Self-practice/self-reflection (SP/SR) training for compassion-focused therapists. In P. Gilbert & G. Simos (Eds.), Compassion focused therapy: Clinical practice and applications (pp. 371–384). Routledge. https://doi.org/10.
Gilbert, P., & Simos, G. (Eds.), Compassion focused therapy: Clinical practice and applications (pp. 371–384). Routledge.
Horwood, V., Allan, S., Goss, K., & Gilbert, P. (2020). The development of the compassion focused therapy therapist competence rating scale. Psychology and Psychotherapy: Theory, Research and Practice, 93(2), 387-407.
Kolts, R. L. (2016). CFT made simple: A clinician's guide to practicing compassion-focused therapy. New Harbinger Publications.
Kolts, R. L., Bell, T., Bennett-Levy, J., & Irons, C. (2018). Experiencing compassion-focused therapy from the inside out: A self-practice/self-reflection workbook for therapists. Guilford Publications.
Liddell, A. E., Allan, S., & Goss, K. (2017). Therapist competencies necessary for the delivery of compassion‐focused therapy: A Delphi study. Psychology and Psychotherapy: Theory, Research and Practice, 90(2), 156-176.
Thwaites, R., & Bennett‐Levy, Melanie Davis and Anna Chaddock, J. (2014). Using Self‐Practice and Self‐Reflection (SP/SR) to Enhance CBT Competence and Metacompetence. How to become a more effective CBT therapist: Mastering metacompetence in clinical practice, 239-254.
Thwaites, R., Cairns, L., Bennett‐Levy, J., Johnston, L., Lowrie, R., Robinson, A., ... & Perry, H. (2015). Developing Metacompetence in Low Intensity Cognitive‐Behavioural Therapy (CBT) Interventions: Evaluating a Self‐Practice/Self‐Reflection Programme for Experienced Low Intensity CBT Practitioners. Australian Psychologist, 50(5), 311-321.
Functional Analytic Psychotherapy (FAP) - Competencies
Functional Analytic Psychotherapy (FAP) - CompetenciesOverview
Functional analytic psychotherapy (FAP)(Kohlenberg &; Tsai, 1987;1991) is a modern,
contextual behavioral psychotherapy that applies behavioral analytic principles to shape client
behavior in the context of a nurturing therapeutic relationship. The proposed mechanism of
change in FAP is the therapist providing appropriate contingent responses to the client’s
clinically relevant behaviors (CRBs) that occur in session. Evidence of FAP’s effectiveness
continues to grow (Kanter et al., 2017) and practitioner interest in learning and using FAP
appears to be growing as well. Assessment of therapist competency in FAP has been an
increased focus as the research on FAP has matured. This section will review existing measures
of FAP competency. For the sake of comprehensiveness, measures of FAP adherence as well as
microprocess-level measures of therapists’ abilities to respond to client behavior with FAP-
consistent responses will also be reviewed. Competency, the ability to appropriately select and
enact FAP-consistent therapist behaviors that are tailored to specific client presentations across
time and across clients, is a more stringently defined class of behavior compared to the classes of
behavior that constitute FAP adherence or FAP-consistent behavior at the microprocess level.
Adherence and microprocess measures might be considered necessary, but not sufficient aspects
of competency. However, since measurement of competency can be resource intense (in terms of
time and complexity of the measurement procedure as well as the time and complexity in the
training of assessors), simpler, pragmatic measures of competency may be useful, particularly
when it is known how they relate to gold standard measures of competency.
Materials/Assessments/Work Products
FAP competencies organized by ACLB (awareness, courage, love, and behaviorism) model
and FAP based on process (Tsai, personal communication).
Description: Created by the developers of FAP, the FAP competencies organized by ACLB
measures five general competencies are defined, with 2-10 subcompetencies defined under each
general competency. Four of the general competencies correspond to the awareness, courage,
love, and behaviorism framework described in Tsai et al. (2009). The fifth general competency is
the ability to integrate the FAP skills in the “logical” FAP interaction (Weeks et al., 2012).
Competencies are collaboratively scored on a five point scale (1=poor; 5=excellent) with
competency being defined as scores of three (good) or above.
FAP Competency Scale (FAPCS) (Kanter, personal communication; Maitland et al., 2016a)
Description: The FAPCS, like the ACLB, is a way to operationalize a measure of competency
that was informed by the comprehensive training vision of the FAP co-developers. The FAPCS
is a 12-item scale developed by a FAP expert (in collaboration with other FAP experts including
the FAP co-developers). The scale includes four items measuring “generalized repertoires” of
awareness, courage, love, and behavioral theory. Eight items measure specific competencies
(assessing CRB, evoking CRBs, appropriate self-disclosure, responding to problematic client
behavior [“CRB1s”], responding to improved client behavior [“CRB2s”], tracking impact of
therapist’s attempts to use reinforcement, providing and shaping functional interpretations
[“CRB3s”], and implementing generalization through homework assignments) that map onto the
five principal FAP rules (Kohlenberg &; Tsai, 1991). Trained coders score recorded therapy
sessions using a four point scale (0=no indication of the behavior at all in the session; 3=a full,
highly competent repertoire displayed in the session). The minimum threshold for FAP
competency is set at a score of 2. Since CRBs are idiographically defined based on the case
conceptualization, the FAPCS is ideally used when the case conceptualization is provided;
however, the FAPCS can be scored without a case conceptualization.
FAP Vignettes (Kanter et al., 2013).
Description: Two brief vignettes are presented followed by prompts for open-ended responses by
trainees. Two items are based on the first vignette, which is a 13 line transcript in which a client
expresses nervousness in response to a therapist’s question. Item one asks trainees to give a FAP-
informed therapist response to the client’s nervousness. Item two asks trainees to provide a brief
FAP rationale to the client. The second vignette presents a single client utterance that trainees are
told to assume represents a clinical improvement (CRB2). The third item measures the extent to
which trainees offer a FAP-consistent response to this CRB2. Items are scored an academic scale
ranging from an F to an A+, which is converted to a numerical scale (F = 0 to A+ = 12) to permit
statistical comparison. The three items are averaged to provide an overall score. Reliability
assessed by a second coder was high (ICCs ranging from 0.88-0.91 for the items).
FAP Impact Scale (FAPIS) (Kanter et al., 2012; Muñoz-Martínez et al., 2024)
Original Article and Scale. Spanish adaptation: Article and Repository.
Description: The FAPIS is a self-report scale with 46 items measuring the impact of FAP
training on trainees. A sample item is “I say things that are hard to say to my clients.” Items are
scored on a 7-point scale (1=”disagree strongly, 4=””neutral/mixed”, 7=”agree strongly”).
Kanter et al. (2012) describe pilot data on the reliability and validity of the scale with two
cohorts (n=10 each) of graduate students. In the study, FAPIS total score had internal
consistency α=0.94. Muñoz-Martínez et al. (2024) reported a replication of the FAP Impact Scale with Spanish-speakers.
FAP Rating Scale (FAPRS)(Callaghan & Follette, 2008; Callaghan & Ruckstuhl, 2000;
Callaghan et al. 2005; Callaghan et al., 2008)
Article and Manual
Description: The FAPRS is a manualized coding system that categorizes client and therapist
statements (turns) on a turn-by-turn basis based on the functional (rather than topographic)
properties of the statements. Callaghan and Follette (2008) state that the FAPRS is “designed to
be functional, or at least quasi-functional with respect to the codes that are assigned to each
client or therapist behavior.” (p. 62). Coders assess the apparent functions of a statement based
on an established FAP case conceptualization. Therefore, the same statement made in a different
client-therapist dyad may be coded differently based on the specific case conceptualization for
each client. Callaghan and Follette (2008) described seven possible codes for client statements
(e.g., CRB2 is a clinically relevant behavior that reflects an in session improvement per the case
conceptualization). Therapist statements are categorized as one of 15 possible codes. Coders are
instructed not to code what the therapist attempts to do but rather whether those attempts are
successful or not. In some applications of the FAPRS, certain codes are combined or omitted for
strategic analytic purposes. A coding hierarchy establishes the priority rules when a statement
appears to contain more than one codable response. For example, if a turn reflects both
problematic in-session behavior and improved in-session behavior, it would be coded as an
improved in-session behavior (CRB2). Since the functional impact of a statement needs to be
assessed in context of the behavior that precedes and follows it, certain codes require an
appropriate antecedent behavior (e.g., a therapist effectively responding to a CRB1, coded as
TCRB1, can only occur in response to a client’s CRB1). To identify the function of a response,
coders can consider the six turns (three statements by the client, three by the therapist) that
follow a statement before deciding how to code that statement.
Therapist In Session Strategies Scale (THISS) (Kohlenberg et al., 2002; Parker, 2006; Parker
et al., 1996)
Description: The THISS consists of 36 items that are divided into four content subscales:
Cognitive Therapy, In Vivo Cognitive Therapy, FAP, and Interpersonal Therapy. The FAP
subscale measures in vivo interventions specific to FAP (e.g., therapist disclosure of thoughts or
feelings about the client’s in vivo behavior).
FAP Adherence Scale (Maitland & Gaynor, 2016)
Description: The FAP Adherence Scale is a 10 item measure with four items comprising a
supportive listening subscale, five items related to application of FAP rules comprising a FAP
subscale, and one item measuring homework assignment. Items 1-9 are scored from 0 (did not
occur) to 3 (occurred three or more times). The homework item is scored as 0 (did not occur, 1
(partial) or 2 (occurred).
Functional Assessment of Skills for Interpersonal Therapists (FASIT) (Callaghan, 2006b)
Description: The FASIT is a detailed manual describing five general classes of interpersonal
behavior that are proposed to be critical for effective interpersonal therapies, particularly FAP.
The manual describes several examples in each class and provides guidance for a trainee or
supervisor to discriminate effective from ineffective therapist behaviors. An appendix includes
idiographic measures of behavior that therapists may be targeting in their own repertoires.
References
Busch, A. M., Callaghan, G. M., Kanter, J. W., Baruch, D. E., & Weeks, C. E. (2010). The Functional Analytic Psychotherapy Rating Scale: A replication and extension. Journal of Contemporary Psychotherapy, 40, 11-19. doi:10.1007/s10879-009- 9122-8.
Busch, A. M., Kanter, J. W., Callaghan, G. M., Baruch, D. E., Weeks, C. E., & Berlin, K. S. (2009). A micro-process analysis of functional analytic psychotherapy’s mechanism of change. Behavior Therapy, 40, 280-290.
Callaghan, G. M. (2006a). The Functional Idiographic Assessment Template (FIAT) system: For use with interpersonally-based interventions including Functional Analytic Psychotherapy (FAP) and FAP-enhanced treatments. The Behavior Analyst Today, 7(3), 357-398.
Callaghan, G. M. (2006b). Functional Assessment of Skills for Interpersonal Therapists: The FASIT system: For the assessment of therapist behavior for interpersonally-based interventions including Functional Analytic Psychotherapy or FAP-enhanced treatments. The Behavior Analyst Today 7(3): 399-433.
Callaghan, G. M., & Follette, W. C. (2008). FAPRS manual: manual for the Functional Analytic Psychotherapy Rating Scale (FAPRS). Behavior Analyst Today, 9, 57-97.
Callaghan, G., & Follette, W. (2020). Interpersonal Behavior Therapy (IBT), Functional Assessment, and the Value of Principle-Driven Behavioral Case Conceptualizations. The Psychological Record, OnlineFirst, 1-11.
Callaghan, G. M., Follette, W. C., Ruckstuhl, L. E., & Linnerooth, P. J. N. (2008). The Functional Analytic Psychotherapy Rating Scale: A behavioral psychotherapy coding system. Behavior Analyst Today, 9, 98-116.
Callaghan, G. M., & Ruckstuhl, L. E. (2000). Manual for the functional analytic psychotherapy rating scale (version 2). Unpublished manual.
Callaghan, G. M., Ruckstuhl, L. E., & Busch, A. M. (2005). Manual for the Functional Analytic Psychotherapy Rating Scale (version 3). Unpublished manual. San José State University, San Jose, CA.
Callaghan, G. M., Summers, C. J., & Weidman, M. (2003). The treatment of histrionic and narcissistic personality disorder behaviors: A single-subject demonstration of clinical improvement using functional analytic psychotherapy. Journal of contemporary psychotherapy, 33(4), 321-339.
Esparza Lizarazo, N. E., Muñoz-Martínez, A. M., Santos, M. M., & Kanter, J. W. (2015). A within-subjects evaluation of the effects of functional analytic psychotherapy on in-session and out-of-session client behavior. The Psychological Record, 65(3), 463-474.
Find a FAP supervisor (n.d.). Functional analytic psychotherapy. Retrieved August 4, 2020, from https://functionalanalyticpsychotherapy.com/find-a-fap-supervisor/.
Kanter, J. W., Landes, S. J., Busch, A. M., Rusch, L. C., Brown, K. R., Baruch, D. E., & Holman, G. I. (2006). The effect of contingent reinforcement on target variables in outpatient psychotherapy for depression: A successful and unsuccessful case using functional analytic psychotherapy. Journal of applied behavior analysis, 39(4), 463-467.
Kanter, J. W., Manbeck, K. E., Kuczynski, A. M., Maitland, D. W., Villas-Bôas, A., &; Ortega,
M. A. R. (2017). A comprehensive review of research on functional analytic
psychotherapy. Clinical Psychology Review, 58, 141-156.
Kanter, J. W., Tsai, M., Holman, G., & Koerner, K. (2013). Preliminary data from a randomized pilot study of web-based functional analytic psychotherapy therapist training. Psychotherapy, 50(2), 248.
Keng, S. L., Waddington, E., Lin, X. B., Tan, M. S. Q., Henn‐Haase, C., & Kanter, J. W.
(2017). Effects of functional analytic psychotherapy therapist training on therapist factors among
therapist trainees in Singapore: A randomized controlled trial. Clinical psychology &; psychotherapy, 24(4), 1014-1027.
Knott, L. E., Wetterneck, C. T., Norwood, W., & Bistricky, S. L. (2019). The impact of training in functional analytic therapy on therapists’ target behavior. Behavior Analysis: Research and Practice, 19(2), 164.
Kohlenberg, R. J., Kanter, J. W., Bolling, M. Y., Parker, C. R., & Tsai, M. (2002). Enhancing cognitive therapy for depression with functional analytic psychotherapy: Treatment guidelines and empirical findings. Cognitive and Behavioral Practice, 9(3), 213-229.
Kohlenberg, R.J., & Tsai, M. (1987). Functional analytic psychotherapy. In N. S. Jacobson (Ed.), Psychotherapists in clinical practice: Cognitive and behavioral perspectives (pp. 388-443). New York: Guilford Press.
Kohlenberg, R. J., & Tsai, M. (1991). Functional analytic psychotherapy: Creating intense and curative therapeutic relationships. Plenum Press. https://doi.org/10.1007/978-0-387-70855-3
Landes, S. J., Kanter, J. W., Weeks, C. E., & Busch, A. M. (2013). The impact of the active components of functional analytic psychotherapy on idiographic target behaviors. Journal of Contextual Behavioral Science, 2(1-2), 49-57.
Maitland, D. W., & Gaynor, S. T. (2016). Functional analytic psychotherapy compared with supportive listening: An alternating treatments design examining distinctiveness, session evaluations, and interpersonal functioning. Behavior Analysis: Research and Practice, 16(2), 52-64.
Maitland, D. W., Kanter, J. W., Tsai, M., Kuczynski, A. M., Manbeck, K. E., & Kohlenberg, R J. (2016a). Preliminary findings on the effects of online Functional Analytic Psychotherapy training on therapist competency. The Psychological Record, 66(4), 627-637.
Maitland, D. W., Petts, R. A., Knott, L. E., Briggs, C. A., Moore, J. A., & Gaynor, S. T. (2016b). A randomized controlled trial of functional analytic psychotherapy versus watchful waiting: Enhancing social connectedness and reducing anxiety and avoidance. Behavior Analysis: Research and Practice, 16(3), 103-122.
Muñoz-Martínez, A. M., Márquez-Barraquer, V., Jiménez-Leal, W., Carmona-Díaz, G. M., & Acuña-Rojas, D. (2024). Assessing the Psychometric Properties of the Functional Analytic Psychotherapy Intimacy Scale (FAPIS) in a Spanish-Speaking Population. The Psychological Record, 1-11.
Novoa-Gómez, M., Córdoba-Salgado, O., Rojas, N., Sosa, L., Cifuentes, D., & Robayo, S. (2019). A descriptive analysis of the interactions during clinical supervision. Frontiers in Psychology, 10, 1-8.
Oshiro, C. K. B., Kanter, J. W., & Meyer, S. B. (2012). A single-case experimental demonstration of functional analytic psychotherapy with two clients with severe interpersonal problems. International Journal of Behavioral Consultation and Therapy, v7 n2-3 p111-116.
Parker, C. R. (2006). Is there a therapist in the house? Measuring in-vivo therapist strategies
during FAP -enhanced cognitive therapy for depression. Dissertation: University of Washington
Parker, C. R., Bolling, M. Y., & Kohlenberg, R. J. (1996) Therapist In-vivo strategy scale. Unpublished manuscript.
University of Washington, Seattle.
Tsai, M., Kohlenberg, R. J., Kanter, J. W., Kohlenberg, B., Follette, W. C., & Callaghan, G. M. (2009). A guide to functional analytic psychotherapy. Awareness, courage, love and behaviorism. New York: Springer.
Vandenberghe, L. (2009). A functional analytic approach to group psychotherapy. The Behavior
Analyst Today, 10(1), 71-82.
Weeks, C. E., Kanter, J. W., Bonow, J. T., Landes, S. J., & Busch, A. M. (2012). Translating the theoretical into practical: A logical framework of functional analytic psychotherapy interactions for research, training, and clinical purposes. Behavior Modification, 36(1), 87-119.
Internet-based Interventions - Competencies
Internet-based Interventions - CompetenciesOverview
Rapid progress in technology has diversified the way behavior change methods such as psychotherapy or coaching are provided. The global movement to limit face-to-face contact caused by the COVID-19 pandemic has accelerated the provision of behavior change methods delivered via the internet. As an example, Cognitive Behavioral Therapy (CBT) has been adapted in various ways. Therapy materials, video clips, and worksheets are provided online, and symptom questionnaires and self-assessments are used to monitor progress as usual but these may be collected and scored in different formats. Generally speaking, there are two types of remote CBT provision. First, clients practice CBT without the support of a therapist. Second, a therapist supports a client by using a remote method such as an online meeting, mail, chat, and telephone. VR has also been used to provide CBT (Maheu, Pulier, McMenamin, & Posen, 2012).
Terminology
Psychological services or interventions provided via the internet have been described in the literature with a variety of terms including "telepsychological services," "Digital mental health technology," "web-based," "Internet CBT," and "tele-CBT." Another complication is that internet-based interventions have sometimes been described as "telehealth" yet the term telehealth has been used in multiple ways, sometimes referring to the provision of psychological services specifically and sometimes referring more generally to both medical and behavioral health interventions. This proliferation of terms has been called “terminology chaos (Barak, 2013). Term reduction is required to evaluate the effectiveness and tasks of remote psychological services or interventions (Andersson, Titov, Dear, Rozental, & Carlbring, 2019). Here we use Internet CBT (ICBT) to represent all types of remote CBTs.
Benefits
Internet-based psychological interventions, including ICBT, have significant advantages over face-to-face psychological services or interventions in terms of time, effort, and costs. A client can choose a good therapist without considering distance, even in a different country (subject to country-specific laws and profession-specific regulations). Internet-based services can be delivered to people with mobility difficulties, such as severe physical disability. Remote delivery of services offers an advantage to clinical research as well since much more participants can be recruited beyond geographical barriers (Andersson, et al., 2019), which may lead to more diverse research samples.
Issues
Data security is crucial, especially when sensitive information is exchanged. Legal requirements for managing personal data are being developed in many countries, and ICBT guidelines are also being provided by the American Psychological Association (Joint Taskforce for the Development of Telepsychology Guidelines for Psychologists, 2013) and Canada (Johnson, 2014). Older persons who are not familiar with using a computer and smartphone and people living in unavailable areas or countries would not be able to benefit from ICBT. The gap in dissemination has widened. Finally, the acceptance of ICBT by insurance companies depends on their country (Andersson et al., 2019).
Current evidence base
Many studies have investigated the effectiveness of ICBT. Recent meta-analyses have shown that ICBT is more effective than no treatment, and therapist-supported ICBT is the same as face-to-face CBT (Cuijpers, Cristea, Karyotaki, Reijnders, & Huibers, 2016; Cuijpers et al., 2009; Spek et al., 2007). A study comparing ICBT with and without therapist support showed that ICBT with support was more effective than that without support for anxiety disorders and depressions (Andrews et al., 2018; Olthuis, Watt, Bailey, Hayden, & Stewart, 2016; Sijbrandij, Kunovski, & Cuijpers, 2016). However, it should be noted that the quality of the evidence was low to moderate (Olthuis et al., 2016).
Trindade et al. (2021) completed a systematic review and meta-analysis of online-based delivery of ACT specifically for chronic pain. Online ACT demonstrated more effectiveness (relative to control conditions) on outcome measures of pain interference, pain intensity, depression, anxiety, mindfulness, and psychological flexibility.
CBS therapies delivered via the internet
Regarding therapies under the rubric of contextual behavior science (CBS), there are some meta-analyses. Most of them focused on Acceptance and Commitment Therapy. The effectiveness or feasibility were reported for subjective wellbeing (Stenhoff, Steadman, Nevitt, Benson, & White, 2020), anxiety (Brown, Glendenning, Hoon, & John, 2016; Kelson, Rollin, Ridout, & Campbell, 2019), and depression (French, Golijani-Moghaddam, & Schröder, 2017; Thompson, Destree, Albertella, & Fontenelle, 2021; Trindade et al., 2021). Lakeman et al. (2022) and van Leeuwen et al. (2021) conducted systematic reviews of DBT provided by the Internet. Lakeman et al. (2022, p.11) reported “current research evidence does not support a permanent shift towards online or blended DBT. It is pivotal and timely to increase efforts to investigate the efficacy of online DBT, compared to standard face-to-face DBT.”
Competency measures
To date, there are limited measures of competency for internet-based interventions. There are several best practice guidelines for the use of telepsychology, which can be used for self-assessment of one's fidelity to the guidelines. For example, see Figure 1 from Maheu et al. (2021) describing telebehavioral health competencies:
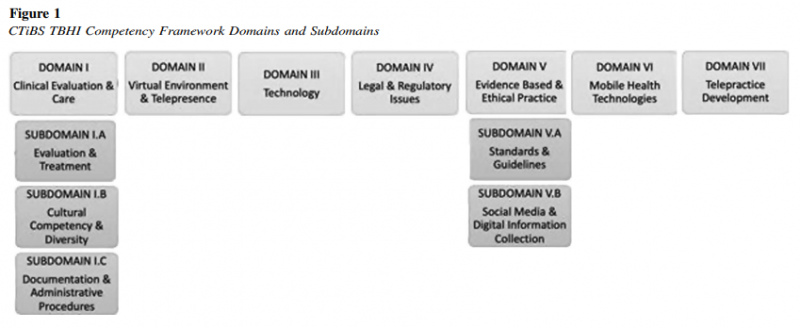
These telepsychology guidelines typically describe ways of effectively delivering services via remote electronic means, and there are meant to apply to a range of psychological interventions spanning a variety of theoretical approaches (e.g., cognitive-behavioral, psychodynamic, humanistic). In a scoping review, McCord et al. (2020) distilled a set of guidelines.
Specific interventions, such as ACT, may have a set of competency measures. Generally, these competencies are not altered when the intervention is delivered remotely. Essentially, practitioners are expected to meet the competencies of telepsychology and the intervention-specific competencies at the same time. As McCord et al (2020) noted: in their discussion of telepsychology competence:
"Most basically, a clinician must first be competent in his or her ability to effectively enact the content of the chosen treatment, regardless of the mode of communication (i.e., telepsychology vs. in‐person). No matter the means of transmitting the services, a provider must be extensively trained and prepared in treatments that they are offering to clients. This includes receiving proper supervision and feedback throughout the training process. For example, a psychologist conducting cognitive behavioral therapy over videoconferencing would not only need to be properly trained in this treatment but also be able to make proper adaptations to treatment based on any available best practices and clinical judgment. An example of an adaptation may be mailing worksheets or sending them over a secure file transfer electronically so that they client is able to follow along and participate in homework. (p. 1076)."
Recently, Weisenmuller & Luzier (2022) called for technology to be considered a core competency for psychologists to develop.
How is culture addressed In the competencies?
Some studies have attempted to adapt or modify ICBT programs developed in Western countries to culturally different countries. Patel et al. (2016) and Abuwalla (2017) adapted the CATCH-IT (Competent Adulthood Transition with Cognitive-Behavioral, Humanistic and Interpersonal Training program), which is an internet-based intervention targeting teens at risk for developing depression, to China and Arabian countries. Zemestani, Hosseini, Petersen, & Twohig (2022) reported internet-based ACT (iACT) in Iran was equally effective as ACT delivered in Western countries. Ramaiya et al.,(2017)provided DBT to persons in Nepal. They conducted the study with three phases. One was qualitative interviews with major Nepali mental health stakeholders, the second was an adaptation workshop with 15 Nepali counselors, and the third was a small-scale treatment pilot with eligible clients in one rural district. They concluded that while DBT concepts were the least comprehensible to clients, the high program completion rate suggested the utility of structured, skills-based treatment of DBT. A systematic review of DBT (Haft, O'Grady, Shaller, & Liu, 2022) revealed that most adaptations involved modifications to language, metaphors, methods, and context, and there was insufficient evidence to determine the effectiveness of culturally adapted DBT. Competency has usually been assessed in these studies by measuring fidelity to the specified intervention. Fidelity measures may include items that address the aim of successfully adapting the intervention to a different cultural context, but competency in doing so is rarely measured.
Willis et al. (2022) made recommendations for increasing the cultural responsivity of telepsychology (and mHealth) interventions, but they did not call for new directions in measures of competence.
How have competencies been operationalized in diverse practice settings and delivery modalities?
Aside from resources on best-practices in delivering therapy through telehealth, no specific guidance was found. McCord et al. (2020) identified key variations in practice settings and delivery modalities for telepsychology, but called for an overall focus on competence and multicultural competence that did not vary across settings.
Materials / Assessments / Work Products
To date, no scale has been developed to measure therapist competency in ICBT. Several guidelines for the implementation of Internet-based telepsychology have been reported, and McCord et al. (2020) summarized them and proposed a practice model. One of the cube models summarizes considerations related to Internet-based psychotherapy (IBT). These are briefly summarized below.
Client appropriateness
Therapists should consider the client's history (e.g., repetitive crises and comfort-receiving telepsychology services). In particular, clients receiving telepsychology services, as opposed to in-person services, are in a situation where self-harm and other behaviors are difficult to control. It is also necessary
to consider the appropriateness of a client's literacy regarding technology.
Informed consents
Therapists should obtain informed consent about the risks, benefits, and alternatives to telepsychology services.
Professional boundaries
Therapists should maintain professional language through email and texting communications. They should clarify that these messages are for the client only and are not shared with others. Therapists should be mindful of the ubiquitous nature of social media and should maintain boundaries by not contacting clients through social media. Therapists should explain to clients their social media policy (e.g., not becoming friends on social media) at the start of the service.
Privacy and confidentiality
Therapists should develop policies regarding security issues (including the use of encryption, transmission, storage, and disposal). Therapists should clearly explain to clients that digital information such as telephone records, videos, and emails is protected and will not be shared outside the organization.
Managing outages and downtime,
Therapists should ensure that the system reliably provides services. At the same time, they should consider that it is inevitable that the system will fail and make plans for this.
Competent
Therapists should be competent in the interventions they provide, regardless of the mode in which the service is provided, for example, telepsychology vs. in-person. This includes receiving ongoing SV. Therapists delivering CBT through videoconferencing should also adapt their in-person interventions, for example, by sending worksheets to clients via secure file transfers.
Termination of services
Therapists should ask clients to assess their satisfaction and the quality of the services provided if the termination of services is deemed appropriate.
Dissemination and maintenance of competencies
Implementation of internet-based interventions has been studied (see e.g., Benavides-Vaello, Strode, & Sheeran, 2013; Jang-Jaccard, Nepal, Alem, & Li, 2014), and the adoption of best-practices has also been described, particularly in the context of the Covid-19 pandemic (Alqahtani et al., 2021; Dopp et al., 2020; Penney et al., 2021) Little is known about the maintenance of competencies specific to internet-based interventions.
References
Abuwalla, Z., Kadhem, Z., Gladstone, T., Mikhael, E., Bishay, A., & Van Voorhees, B. W. (2017). Proposed model for the cultural adaptation of an Internet-based depression prevention intervention (CATCH-IT) for Arab adolescents. International Journal of Adolescent Medicine and Health, 31(1), 20160147.
Alqahtani, M. M. J., Alkhamees, H. A., Alkhalaf, A. M., Alarjan, S. S., Alzahrani, H. S., AlSaad, G. F., ... & Alqahtani, K. M. M. (2021). Toward establishing telepsychology guideline. Turning the challenges of COVID-19 into opportunity. Ethics, Medicine and Public Health, 16, 100612.
Andersson, G., Titov, N., Dear, B. F., Rozental, A., & Carlbring, P. (2019). Internet‐delivered psychological treatments: from innovation to implementation. World Psychiatry, 18(1), 20-28.
Andrews, G., Basu, A., Cuijpers, P., Craske, M., McEvoy, P., English, C., & Newby, J. (2018). Computer therapy for the anxiety and depression disorders is effective, acceptable and practical health care: an updated meta-analysis. Journal of anxiety disorders, 55, 70-78.
Barak, A. (2013). Concepts, definitions, and applications: the terminology cha os of Internetsupported psychotherapeutic interventions. Paper presented at the 6th Meeting of the International Society for Research on Internet Interventions, Chicago.
Benavides-Vaello, S., Strode, A., & Sheeran, B. C. (2013). Using technology in the delivery of mental health and substance abuse treatment in rural communities: a review. The journal of behavioral health services & research, 40(1), 111-120.
Brown, M., Glendenning, A., Hoon, A. E., & John, A. (2016). Effectiveness of web-delivered acceptance and commitment therapy in relation to mental health and well-being: a systematic review and meta-analysis. Journal of medical Internet research, 18(8), e221.
Cuijpers, P., Cristea, I. A., Karyotaki, E., Reijnders, M., & Huibers, M. J. (2016). How effective are cognitive behavior therapies for major depression and anxiety disorders? A meta‐analytic update of the evidence. World Psychiatry, 15(3), 245-258.
Cuijpers, P., Marks, I. M., van Straten, A., Cavanagh, K., Gega, L., & Andersson, G. (2009). Computer‐aided psychotherapy for anxiety disorders: A meta‐analytic review. Cognitive Behaviour Therapy, 38(2), 66-82.
Dopp, A. R., Mapes, A. R., Wolkowicz, N. R., McCord, C. E., & Feldner, M. T. (2021). Incorporating telehealth into health service psychology training: A mixed-method study of student perspectives. Digital health, 7, 2055207620980222.
Joint Taskforce for the Development of Telepsychology Guidelines for Psychologists (2013). Guidelines for the practice of Telepsychology. The American psychologist, 68(9), 791-800.
French, K., Golijani-Moghaddam, N., & Schr?der, T. (2017). What is the evidence for the efficacy of self-help acceptance and commitment therapy? A systematic review and meta-analysis. Journal of Contextual Behavioral Science, 6(4), 360-374.
Haft, S. L., O'Grady, S. M., Shaller, E. A., & Liu, N. H. (2022). Cultural adaptations of dialectical behavior therapy: A systematic review. Journal of consulting and clinical psychology.
Jang-Jaccard, J., Nepal, S., Alem, L., & Li, J. (2014). Barriers for delivering telehealth in rural Australia: a review based on Australian trials and studies. Telemedicine and e-Health,?20(5), 496-504.
Johnson, G. R. (2014). Toward uniform competency standards in telepsychology: A proposed framework for Canadian psychologists. Canadian Psychology/Psychologie canadienne, 55(4), 291.
Kelson, J., Rollin, A., Ridout, B., & Campbell, A. (2019). Internet-delivered acceptance and commitment therapy for anxiety treatment: systematic review. Journal of medical Internet research, 21(1), e12530.
Lakeman, R., King, P., Hurley, J., Tranter, R., Leggett, A., Campbell, K., & Herrera, C. (2022). Towards online delivery of Dialectical Behaviour Therapy: A scoping review. International Journal of Mental Health Nursing, 31(4), 843-856.
Maheu, M. M., Pulier, M. L., McMenamin, J. P., & Posen, L. (2012). Future of telepsychology, telehealth, and various technologies in psychological research and practice. Professional psychology: Research and practice, 43(6), 613.
Maheu, M. M., Wright, S. D., Neufeld, J., Drude, K. P., Hilty, D. M., Baker, D. C., & Callan, J. E. (2021). Interprofessional telebehavioral health competencies framework: Implications for telepsychology. Professional Psychology: Research and Practice, 52(5), 439.
McCord, C., Bernhard, P., Walsh, M., Rosner, C., & Console, K. (2020). A consolidated model for telepsychology practice. Journal of Clinical Psychology, 76(6), 1060-1082.
Olthuis, J. V., Watt, M. C., Bailey, K., Hayden, J. A., & Stewart, S. H. (2016). Therapist‐supported Internet cognitive behavioural therapy for anxiety disorders in adults. Cochrane Database of Systematic Reviews(3).
Patel, U., Sobowale, K., Fan, J., Liu, N., Kuwabara, S., Lei, Z., . . . Van Voorhees, B. (2016). Cultural considerations for the adaptation of an Internet-based intervention for depression prevention in Mainland China. International Journal of Adolescent Medicine and Health, 29(5), 20150099.
Penney, E., Reynolds, J., Knott, V., & Green, H. (2022). Lessons from 2020: practical and clinical aspects of rapid telepsychology adoption in clinical psychology postgraduate programs. Australian Psychologist, 57(3), 161-166.
Ramaiya, M. K., Fiorillo, D., Regmi, U., Robins, C. J., & Kohrt, B. A. (2017). A cultural adaptation of dialectical behavior therapy in Nepal. Cognitive and Behavioral Practice, 24(4), 428-444.
Sijbrandij, M., Kunovski, I., & Cuijpers, P. (2016). Effectiveness of internet‐delivered cognitive behavioral therapy for posttraumatic stress disorder: A systematic review and meta‐analysis. Depression and anxiety, 33(9), 783-791.
Spek, V., Cuijpers, P., Nykl??ek, I., Riper, H., Keyzer, J., & Pop, V. (2007). Internet-based cognitive behaviour therapy for symptoms of depression and anxiety: a meta-analysis. Psychologicalmedicine, 37(3), 319-328.
Stenhoff, A., Steadman, L., Nevitt, S., Benson, L., & White, R. G. (2020). Acceptance and commitment therapy and subjective wellbeing: A systematic review and meta-analyses of randomised controlled trials in adults. Journal of Contextual Behavioral Science, 18, 256-272.
Thompson, E. M., Destree, L., Albertella, L., & Fontenelle, L. F. (2021). Internet-based acceptance and commitment therapy: a transdiagnostic systematic review and meta-analysis for mental health outcomes. Behavior therapy, 52(2), 492-507.
Trindade, I. A., Guiomar, R., Carvalho, S. A., Duarte, J., Lapa, T., Menezes, P., . . . Castilho, P. (2021). Efficacy of online-based acceptance and commitment therapy for chronic pain: A systematic review and meta-analysis. The Journal of Pain, 22(11), 1328-1342.
van Leeuwen, H., Sinnaeve, R., Witteveen, U., Van Daele, T., Ossewaarde, L., Egger, J. I., & van den Bosch, L. (2021). Reviewing the availability, efficacy and clinical utility of Telepsychology in dialectical behavior therapy (Tele-DBT). Borderline personality disorder and emotion dysregulation, 8(1), 1-15.
Weisenmuller, C. M., & Luzier, J. L. (2022). Technology is a core competency in professional psychology. Training and Education in Professional Psychology.
Willis, H. A., Gonzalez, J. C., Call, C. C., Quezada, D., Scholars for Elevating Equity and Diversity (SEED), & Galán, C. A. (2022). Culturally Responsive Telepsychology & mHealth Interventions for Racial-Ethnic Minoritized Youth: Research Gaps and Future Directions. Journal of Clinical Child & Adolescent Psychology, 51(6), 1053-1069.
Zemestani, M., Hosseini, M., Petersen, J. M., & Twohig, M. P. (2022). A pilot randomized controlled trial of culturally-adapted, telehealth group acceptance and commitment therapy for Iranian adolescent females reporting symptoms of anxiety. Journal of Contextual Behavioral Science, 25, 145-152.
Mindfulness Approaches - Competencies
Mindfulness Approaches - CompetenciesCompetency Measurement in Mindfulness
Mindfulness has grown in popularity as both a practice and an intervention. Research assessing the impact of mindfulness practice has also surged in more recent years, with benefits ranging from reduced rumination (Chambers, et al., 2008) to stress reduction (Hoffman et al., 2010) to less emotional reactivity (Ortner, et al., 2007) and more cognitive flexibility (Cahn & Polich, 2006; Davidson et al., 2003; Siegel, 2007). It has also been shown to support therapists by improving empathy (Aiken, 2006), compassion (Kingsbury, 2009), and counseling skill (Newsome, et al., 2006; Schure, et al., 2008). Scores of other benefits are found in the research literature (for a review, see Goldberg, et al, 2018 for a review).
Despite this growth, little research has been conducted on competencies for those who implement or use mindfulness as a therapeutic approach. However, underlying philosophy and stages of competence have been defined (see Dreyfus and Dreyfus 1986), and a call to competency in delivering this practice has been made: “In this rapidly developing context, there is a growing demand for teachers and trainers of teachers. Understandably, concerns are being expressed from within the field that practitioners may be tempted to respond to this demand without engaging in personal preparation and developing the competencies required for these endeavors (e.g., Crane et al., 2012).” One study evaluating 16 mindfulness competencies has also been conducted (Stauffer & Pehrsson, 2012), and competencies in teaching mindfulness-based courses have been explored (Crane, et al., 2011). Recent efforts to provide competency guidelines for clinical social workers have underscored the importance of focusing on the competent delivery of mindfulness training and practice (Paulson, 2018).
It is important to recognize that several of the CBS-oriented therapies use mindfulness practices as a part of their interventions and has been included in information concerning intervention-specific competencies. For instance, acceptance and commitment therapy acknowledges mindfulness practices in two of its core process competencies: 1) Present Moment: The therapist uses exercises to expand the client’s sense of experience as an ongoing process (e.g., mindfulness exercises), and 2) Self-as-context: The therapist helps the client make a distinction between self as context and content by employing mindfulness exercises (e.g., leaves on a stream, soldiers on parade, observer exercise) metaphors (e.g., chessboard) and behavioral tasks (e.g., take your mind for a walk). Consideration in mindfulness competencies is relevant to the CBS-oriented therapies using this practice.
Products/Assessments/Work Products
Adaptation of Dreyfus and Dreyfus stages of competence (see Dreyfus and Dreyfus 1986 or Crane et al., 2011) for mindfulness-based teaching competence:
Summary of Competence and the Underlying Philosophy of Mindfulness-Based Approaches
List of Competencies to train clients in mindfulness methods
1. Regular daily practice
2. Educational resources on mindfulness
3. Therapeutic alliance
4. Meta-cognitive awareness
5. Empathy
6. Facing rather than avoiding difficult experiences
7. Attention regulation
8. Acceptance and non-judgement
Stage Competence descriptors:
1. Incompetent Teaching:
Is inappropriate, likely to compromise the safety of participants, and to lead to negative therapeutic consequences. The trainee has not grasped the fundamentals of mindfulness-based teaching practice and does not recognize basic principles and rules. There is nonadherence to the program form.
2. Beginner Trainees:
Operate in a state of rule learning and rule governedness. Preparation for teaching is likely to be dominated by memorizing scripted responses to participants and bringing to mind a list of ‘teaching points’ to bring to class dialogues. Although aspects of competence are demonstrated at this stage, there are numerous substantive problems and an overall lack of consistency. Experience is needed to progress through this stage—underlining the importance of training programs offering considerable time to practice skills with fellow trainees and receive feedback.
3. Advanced beginner:
Having had opportunities to practice newly acquired skills in mindfulness-based teaching, trainees are able to more easily recall the ‘rules’ that need applying (i.e. the different steps within the sitting practice guidance, ways of opening up class dialogue following a practice) and are increasingly able to apply these in a more sophisticated way. The teaching process is still deliberative, and significant inconsistencies require further development, but competencies are clearly demonstrated. Participants’ emotional and physical safety is adequately taken care of, and at a very basic level, the teacher is ‘fit for practice’—at this stage, the participants would not be harmed and are likely to have opportunities for learning.
4. Competent:
Focusing on context-free rules in the previous stages drains attentional resources and, through increasing familiarity with the teaching process becomes far less necessary. Trainees at this stage move away from a predominant focus on applied problem solving and the application of learned rules towards an embodied engagement in the moment and a greater degree of fluid responsiveness. Although there are some inconsistencies and problems, the teaching is at a workable level of competence and is clearly ‘fit for practice’.
5. Proficiency:
At this stage, the teacher can intuitively use learned patterns without decomposing them into component features and has increased moment-by-moment responsiveness and flexibility. The teacher operates from direct contact with the arising of experience in self, in individual participants, and in the group.
6. Advanced:
At this stage, the skill that the teacher has in teaching mindfulness is part of him/her as a person. While teaching, they are immersed in the process and no longer use rules, guidelines, or maxims. She/he has a deep tacit understanding of the teaching and is an original, flexible, and fluid teacher. The breadth and depth of knowledge of the teacher at this developmental stage is an inspiration to others. At this stage, the teacher’s skills are consistent despite strong difficulties such as participant hostility or strong emotion. The process is intuitive, and the teacher is unlikely to be able to articulate how he/she is teaching if asked easily.
https://link.springer.com/article/10.1007/s12671-011-0073-2/tables/1
Methodologies for assessing mindfulness teaching skills associated with competence: Teaching portfolios
1. Reflective assignments
2. Academic assignments
3. Self-assessment
4. Peer assessment
5. Review of teaching by an expert panel
6. Use of rating scales: two scales: The MBCT Adherence scale
7. Mindfulness-based Relapse Prevention Adherence and Competence Scale
https://link.springer.com/article/10.1007/s12671-011-0073-2/tables/2
____________________
| Table 1: General Guidelines of Developing Competency with Mindfulness-Based Interventions |
|---|
| 1. Baseline general clinical competency |
| 2. Functional understanding of mindfulness |
| 3. Training in the delivery of mindfulness skills |
| 4. On-going supervision and education related to mindfulness |
| 5. Sensitivity to diversity issues and client preference |
| 6. The clinician maintaining their own personal mindfulness practice |
Paulson, J. (2018). Developing competence with mindfulness-based interventions: Guidelines for clinical social workers. Journal of Sociology and Social Work, 6(1), 1-6:
References
Aiken, G. A. (2006). The potential effect of mindfulness meditation on the cultivation of empathy in psychotherapy: A qualitative inquiry (Doctoral dissertation, Saybrook University).
Britton, W. B. (2016). Scientific literacy as a foundational competency for teachers of mindfulness-based interventions. Resources for teaching mindfulness: An international handbook, 93-119.
Cahn BR, Polich J. Meditation states and traits: EEG, ERP, and neuroimaging studies. Psychol Bull. 2006;132:180–211
Chambers, R., Lo, B. C. Y., & Allen, N. B. (2008). The impact of intensive mindfulness training on attentional control, cognitive style, and affect. Cognitive therapy and research, 32, 303-322.
Crane, R. S., Kuyken, W., Williams, J. M. G., Hastings, R. P., Cooper, L., & Fennell, M. J. (2012). Competence in teaching mindfulness-based courses: concepts, development and assessment. Mindfulness, 3, 76-84.
Crane, R. S., Soulsby, J. G., Kuyken, W., Williams, J. M. G., & Eames, C. (2011). The Bangor, Exeter &Oxford mindfulness-based interventions: teaching assessment criteria. Unpublished manuscript.
Davidson, R. J., Kabat-Zinn, J., Schumacher, J., Rosenkranz, M., Muller, D., Santorelli, S. F., ... & Sheridan, J. F. (2003). Alterations in brain and immune function produced by mindfulness meditation. Psychosomatic medicine, 65(4), 564-570.
Dreyfus HL, Dreyfus SE. Mind over machine: the power of human intuition and experience in the age of computers. New York: Free Press; 1986.
Goldberg, S. B., Tucker, R. P., Greene, P. A., Davidson, R. J., Wampold, B. E., Kearney, D. J., & Simpson, T. L. (2018). Mindfulness-based interventions for psychiatric disorders: A systematic review and meta-analysis. Clinical psychology review, 59, 52-60.
Kingsbury, E. (2009). The relationship between empathy and mindfulness: Understanding the role of self-compassion. ProQuest Information & Learning.
Masuda, A. (Ed.). (2014). Mindfulness and acceptance in multicultural competency: A contextual approach to sociocultural diversity in theory and practice. New Harbinger Publications.
Newsome, S., Christopher, J. C., Dahlen, P., & Christopher, S. (2006). Teaching counselors self-care through mindfulness practices. Teachers College Record, 108(9), 1881-1900.
Ortner, C. N., Kilner, S. J., & Zelazo, P. D. (2007). Mindfulness meditation and reduced emotional interference on a cognitive task. Motivation and emotion, 31, 271-283.
Paulson, J. (2018). Developing competence with mindfulness-based interventions: Guidelines for clinical social workers. Journal of Sociology and Social Work, 6(1), 1-6.
Schure, M. B., Christopher, J., & Christopher, S. (2008). Mind–body medicine and the art of self‐care: teaching mindfulness to counseling students through yoga, meditation, and qigong. Journal of Counseling & Development, 86(1), 47-56.
Siegel, D. J. (2007). Mindfulness training and neural integration: Differentiation of distinct streams of awareness and the cultivation of well-being. Social cognitive and affective neuroscience, 2(4), 259-263.
Stauffer, M., & Pehrsson, D. E. (2012). Mindfulness competencies for counselors and psychotherapists. Journal of Mental Health Counseling, 34(3), 227-239.
Process-Based Therapy (PBT) - Competencies
Process-Based Therapy (PBT) - CompetenciesOverview
Process-Based Therapy (PBT) has been developed as an alternative to the "protocols for syndromes" approach to diagnosis and treatment. PBT has been described as a return to the functional roots that informed the early practice of behavior therapy (Hofmann and Hayes, 2019). One strand in the development of PBT is a task force report on CBT competencies among doctoral trainees (Klepac et al., 2012). Hayes and Hofmann (2018) elaborated on these CBT competencies from a contextual behavioral science lens that was termed "Process-based CBT." Process-based CBT refers to the use of various change processes identified from mediational research. PBT appears to be a more general form of Process-based CBT that makes more intensive use of an idiographic network diagramming approach (in order to avoid the ergodic error associated with change processes identified from group rather than individual research). Empirical research explicitly focusing on PBT has recently emerged including the development of item pools (Ciarrochi, Sahdra, Hofmann, and Hayes, 2022) and the statistical identification of functional processes that can be interpreted as a case conceptualization (Sanford et al., 2022). PBT is not meant to be considered a specific kind of therapy; rather, it is proposed to be an alternative way to operationalize evidence-based therapy/practice; thus, the use of methods and theories beyond CBT can be accommodated within the PBT approach (although the developers state that the change processes--which may have different names in different clinical traditions--must be empirically-supported "intervention kernels").
Current State of Competencies
Competency in PBT has yet to be formally defined or evaluated. However, the competencies have been described in various publications, and general principles of how PBT competency might be implemented and evaluated are evident from these sources. A few of these publications, most notably the Learning Process-Based Therapy book, include useful work products such as sample network conceptualizations. Additional work products are available on the Processed-Based Therapy SIG listserve.
PBT co-developer Steven C. Hayes (personal communication) described how competency in PBT can be generally conceptualized. Specifically, one must be competent in reading the processes. One must be competent in developing, monitoring, validating, and re-evaluating the dynamic network of processes. One must also be competent in delivering the intervention kernerls that are likely to move the key processes that have been identified by the network analysis.
The development of analytic methods to assist practitioners in the application of these competencies is an active area of development as of July 2023. Digital tools to collect intensive longitudinal data needed to model individual dynamics are in development. A conceptual approach that may help practitioners target relevant processes is the multi-dimensional, multi-level extended evolutionary meta-model (EEMM) (Hayes, Hoffman, and Ciarrochi, 2020). Empirically, the recent review of all replicated measures that mediate psychological outcomes can by organized with the EEMM to identify processes that may be relevant to target and measure (Hayes et al., 2022).
Several intervention kernels are known (see e.g., Hayes and Hoffman, 2018). The efficacy of existing kernels and newly developed kernels is continually being evaluated. Identifying relevant intervention kernels requires practitioners to stay up to date with the empirical status of each kernel (paying particular attention to meta-analyses). Developing competency with specific kernels is outside the scope of PBT. However, PBT may offer a solution to measuring competency with any chosen kernel by virtue of the fact that the individual network must be specified and changes in the network must be measured, which will provide evidence of the impact of the intervention.
Materials/Assessments/Work Products
For a book length treatment specifically describing therapist competencies, see Hofmann, Hayes, and Lorscheid (2021). The book includes free resources.
There is a Processed-Based Therapy Special Interest Group (SIG) that actively discusses PBT skills.
MindGrapher and PLAN (Personalized Life Analysis Network) are commercially available tools to help with conceptualizing cases using a PBT approach.
References
Ciarrochi, J., Sahdra, B., Hofmann, S. G., & Hayes, S. C. (2022). Developing an item pool to assess processes of change in psychological interventions: The Process-Based Assessment Tool (PBAT). Journal of Contextual Behavioral Science, 23, 200-213.
Hayes, S. C., Ciarrochi, J., Hofmann, S. G., Chin, F., & Sahdra, B. (2022). Evolving an idionomic approach to processes of change: Towards a unified personalized science of human improvement. Behaviour Research and Therapy, 156, 104155. Doi: 10.1016/j.brat.2022.104155
Hayes, S. C., & Hofmann, S. G. (Eds.). (2018). Process-based CBT: The science and core clinical competencies of cognitive behavioral therapy. New Harbinger Publications.
Hayes, S. C., Hofmann, S. G. & Ciarrochi, J. (2020). A process-based approach to psychological diagnosis and treatment: The conceptual and treatment utility of an extended evolutionary model. Clinical Psychology Review, 82, 101908. doi: 10.1016/j.cpr.2020.101908
Hayes, S. C., Hofmann, S. G., & Stanton, C. E. (2020). Process-based functional analysis can help behavioral science step up to the challenges of novelty: COVID – 19 as an example. Journal of Contextual Behavioral Science, 18, 128-145. doi: 10.1016/j.jcbs.2020.08.009.
Hayes, S. C., Hofmann, S. G., Stanton, C. E., Carpenter, J. K., Sanford, B. T., Curtiss, J. E., & Ciarrochi, J. (2019). The role of the individual in the coming era of process-based therapy. Behaviour Research and Therapy, 117, 40-53. doi: 10.1016/j.brat.2018.10.005
Hofmann, S. G., & Hayes, S. C. (2019). Functional analysis is dead: Long live functional analysis. Clinical Psychological Science, 7(1), 63-67.
Hofmann, S. G., Hayes, S. C., & Lorscheid, D. N. (2021). Learning process-based therapy: A skills training manual for targeting the core processes of psychological change in clinical practice. New Harbinger Publications.
Klepac, R. K., Ronan, G. F., Andrasik, F., Arnold, K. D., Belar, C. D., Berry, S. L., ... & Strauman, T. J. (2012). Guidelines for cognitive behavioral training within doctoral psychology programs in the United States: Report of the Inter-organizational Task Force on Cognitive and Behavioral Psychology Doctoral Education. Behavior Therapy, 43(4), 687-697.
Sanford, B. T., Ciarrochi, J., Hofmann, S. G., Chin, F., Gates, K. M., & Hayes, S. C. (2022). Toward empirical process-based case conceptualization: An idionomic network examination of the process-based assessment tool. Journal of Contextual Behavioral Science.