Resources for Clinicians
Resources for CliniciansIn keeping with one of the values of ACBS as a society, those who create clinical tools, measures, protocols, or other aids for case conceptualization, prevention or intervention work are asked to share these clinical resources with the society. Therefore, the materials posted here are available to paid ACBS professional or student members. Reciprocity is also key, so please consider sharing with the society any materials you have found useful.
Exercises, protocols, metaphors, visual aids and other materials are always a welcome addition to any clinician's arsenal of techniques.
The resources available here are intentionally non-proprietary, but we recommend emailing the authors to find out more about their preferences for citations, etc.
Also be sure to check out available assessment measures, treatment protocols, and books.
Choose a child page below for the topic of interest to you. To add new content, simply create a child page under the topic most relevant for your information, or create a new child page to add your new material.
Informed Consent for ACT
Informed Consent for ACTIn a recent discussion on the ACT listserve, a member asked about how we handle issues of informed consent in the use of ACT. Below is my own understanding of informed consent:
In my own training and the way I train folks, therapy should always start with informed consent. Below is a thumbnail of my approach:
1) Address alternative therapies
I think it is beholden on us to mention alternative treatment approaches that have demonstrated efficacy (including pharmacotherapy) and also to mention that alternative treatments where the direct evidence base is not substantial, but appears to be sensible given the more general evidence available in the literature. If there is a gold standard, like Barlow's PCT for panic--I tell them about it.
I do not get into any kind of big theoretical discussion about, my reservations about the overselling of pharmacotherapy or my own understanding of the likely mechanisms of action in cognitive therapy. I don't do those therapies and if people want them, I can point them to folks who are well versed in them. I also do discuss allegiance effects, though I take them quite seriously. I think that whenever possible, one ought to get therapy from someone who is fully invested in that sort of work. So, if someone wanted CT for depression, I would be the wrong guy. I know smart capable people who do that sort of treatment and am happy to refer folks to them. Likewise, if someone presents with panic, I am not going to do a straight up PCT treatment with them, even though it is the gold standard. I will tell them about PCT (including that is the gold standard) and say that I would do work that has many similarities and is based on many of the same principles, but if they want that specific treatment, I refer to another provider in our clinic. (See below the section on describing the treatment I do as to some ways it might differ from a straight up PCT protocol.
2) Address risks and benefits
My addressing of risks and benefits does not look much different than risks and benefits for any treatment--i.e. not everyone benefits from any treatment, even the most successful varieties. I do not bury a client in a lit review or a checklist of diagnoses for which there is ACT evidence. I do not really buy the diagnostics much anyway. I typically tell people that the treatment we do is directly connected to a tradition that has been useful for a lot of difficulties and that the evidence for this particular looks very promising in the breadth of difficulties for which it seems useful. I also tell clients that treatment is difficult work. I tell people that they may experience significant distress during treatment. I promise to talk about how the person is doing along the way and if it looks like this treatment is not beneficial, I promise to work with them to find the best alternative treatment referral (since my group only focuses on ACT and behaviorally-oriented work).
3) Propose specific time frame
I generally tell clients that it can be a problem estimating whether treatment is useful on a moment by moment basis. Sometimes I use metaphors to illustrate this point. For example, if you plant a garden, going outside every fifteen minutes to see how it is coming along doesn't work very well. Or, going to the gym to get in shape--sometimes you feel worse physically before you start to see the benefits. Also, like physical training sometimes you see periods of progress punctuated by periods that are somewhat flat. I like to start with a time frame where we will stop and look back and ask ourselves "are we headed in the right direction." Partly the time frame depends on the client and the difficulty, but I like a window of 4-6 weeks. This does not mean I expect life to be peaches and cream in 4-6 weeks, just that I think in that time period we should have some sense that we are headed in a direction that seems to have some vitality.
4) Orient person to therapist, client roles
I tell clients that we will be working from a perspective that sees the people we call clients and the people we call therapists as being in the same boat. The rock climber metaphor from the book is a reasonable approximation of the relationship. I honestly can't recall exactly what is in the book, but like two rock climbers on opposite rock faces, there are things I might be able to see from where I stand that would be hard for them to see--not because I am all wise or something, just because I am standing in a different place. Likewise, there are things they can see and feel that I cannot--like the feel, temperature and texture of the rock. I tell clients that if I am to be most useful to them, it will help if I can see the world through their eyes, feel it with their hands. I can't, but I tell them that I will ask them to do their best to give me a sense of what it is like to live in their skin. And then I follow through. My aim is that a client leaves the room with no doubt that their experience was the most important thing in that room during that session. The combination of my somewhat different perspective and their own felt sense of their situation seems to me like the best shot at finding a way forward that works. I tell them this.
We used to say I will be very active at the beginning and that will lessen later. I tend to say something more like sometimes I will be more active and sometimes you will be.
5) Give general descriptions of operating principles
Since generally, behavioral methods are justifiable given the evidence base (exposure-based work, behavioral activation) I tell people that ACT is based on many of the same principles as the best supported treatments available, and will use many of the same methods, but that it tends to look at difficulties in the broader context of whole lives and an individual's valued directions. Therefore the treatment will end up looking at valued domains of living and the ways that these difficulties fit into that whole life. I generally tell them that the work is acceptance focused and whole life focused, rather than being focused on very specific problems. Problems are not ignored, at all; however, they are looked at in this broader way. I tell them that it will be very, very hard work and that we will not do a bit of work except in the service of the direction they would like to take their lives.
I hope this is useful.
peace,
Kelly G. Wilson
Metaphors
MetaphorsThe purpose of this section is to allow members to share new ACT-relevant metaphors that have come out of their therapeutic or accademic work. If adding a metaphor (by adding a child page), please say something about it. For example, how it might be used or what ACT-relevant points it might be trying to make.
Understanding metaphors in ACT
Understanding metaphors in ACTHere is an article "Metaphors in ACT: Understanding how they work, Using them, and Creating your own" discussing the use of metaphors in ACT, from an RFT perspective, as well as from the perspective of the clinician. This article aims to help practitioners understand RFT in basic terms and to see how it applies directly to clinical work through the creation and use of metaphors. Jean-Louis Monestès and Matthieu Villatte authored the article, and interviewed Yvonne Barnes-Holmes (both a clinician and RFT researcher).
You can also read two books:
- Metaphor in Practice: A Professional's Guide to Using the Science of Language in Psychotherapy by Niklas Törneke M.D.
- The Big Book of ACT Metaphors: A Practitioner's Guide to Experiential Exercises and Metaphors in Acceptance and Commitment Therapy by Jill A. Stoddard Ph.D. and Niloofar Afari Ph.D.
If you are interested in learning more about the creation of metaphor from an RFT perspective, check out Ian Stewart's 2001 paper on the subject.
Understanding, Using, and Creating Metaphors with Relational Frame Perspectives in Acceptance–Commitment Therapy (The Korean Journal of Health Psychology)
Understanding, Using, and Creating Metaphors with Relational Frame Perspectives in Acceptance–Commitment Therapy (The Korean Journal of Health Psychology)전북대학교 (2015). 수용 전념 치료 (ACT)에서 관계 틀 관점으로 은유를 이해하고, 활용하고, 창조하기. 한국심리학회지: 건강, 20(2), 371 - 389. [Son, C.N. (2015). Understanding, Using, and Creating Metaphors with Relational Frame Perspectives in Acceptance–Commitment Therapy. The Korean Journal of Health Psychology, 20(2), 371 - 389.] DOI: 10.17315/kjhp.2015.20.2.001
Metaphors in Languages Other Than English
Metaphors in Languages Other Than English CommunityMetaphors in French (Français)
Metaphors in French (Français)Les Passagers du Bus
Les Passagers du BusLes Passagers du Bus (Français): A French animated Choose Your Own Adventure video series featuring The Passengers On The Bus metaphor. Viewers are able to make decisions that shape the story, with each video demonstrating the impact of their chosen strategy: https://www.youtube.com/watch?v=TYjIYp-46zc
Metaphors in Greek
Metaphors in Greek Communityεπιβάτες στο λεωφορείο
επιβάτες στο λεωφορείοΟι "επιβάτες στο λεωφορείο" είναι μία από τις μεταφορές στη ΘΑΔ που μας υπενθυμίζουν τη σπουδαιότητα της οδήγησης προς τις αξίες μας. Οι επιβάτες αποτελούν τις αρνητικές μας σκέψεις. Για παράδειγμα, αν ετοιμαζόμαστε να πάρουμε ένα ρίσκο, ίσως το μυαλό μας αρχίζει να παράγει σκέψεις όπως "Δεν είμαι αρκετά καλός", "Θα αποτύχω", "Ας μην πάρω το ρίσκο καλύτερα" κλπ. Αν όντως ακούσουμε τις σκέψεις αυτές, πιθανώς να αλλάξουμε γνώμη και κατεύθυνση. Το "κέρδος" σε αυτή την περίπτωση είναι η αίσθηση ότι βάλαμε τους επιβάτες (τις σκέψεις δηλαδή) στη θέση τους και δεν μας ταλαιπωρούν πια από τη θέση του οδηγού. Ωστόσο, οι επιβάτες παραμένουν μες στο λεωφορείο. Η επιλογή του να παραμείνουμε πιστοί στον αρχικό μας στόχο και να αφήσουμε τους επιβάτες να μας μιλάνε, μας βοηθά στην καλλιέργεια της αποδοχής. Δεν θέλουμε να τους κάνουμε να σωπάσουνε ούτε να τους βάλουμε σε συγκεκριμένες θέσεις. Θέλουμε να συνεχίσουμε να έχουμε το τιμόνι στα χέρια μας και να φτάσουμε στον προορισμό μας. Το αληθινό κέρδος εδώ δεν είναι μόνο ότι καταφέραμε να αποδεχτούμε τις σκέψεις, αλλά και ότι δείξαμε δέσμευση στις αξίες μας. Αυτό μας κάνει ψυχολογικά ευέλικτους. Και η ψυχολογική ευελιξία μας επιτρέπει μας οδηγήσουμε κάθε όχημα με κάθε είδος επιβατών.
Metaphors in Italian
Metaphors in ItalianThe ACBS Italy Chapter has metaphor resources on its website.
Metaphors in Korean (한국어)
Metaphors in Korean (한국어) Community수용 전념 치료 (ACT)에서 관계 틀 관점으로 은유를 이해하고, 활용하고, 창조하기
수용 전념 치료 (ACT)에서 관계 틀 관점으로 은유를 이해하고, 활용하고, 창조하기전북대학교 (2015). 수용 전념 치료 (ACT)에서 관계 틀 관점으로 은유를 이해하고, 활용하고, 창조하기. 한국심리학회지: 건강, 20(2), 371 - 389. [Son, C.N. (2015). Understanding, Using, and Creating Metaphors with Relational Frame Perspectives in Acceptance–Commitment Therapy. The Korean Journal of Health Psychology, 20(2), 371 - 389.] DOI: 10.17315/kjhp.2015.20.2.001
Metaphors in Polish (Polski)
Metaphors in Polish (Polski) CommunityDemony na łodzi
Demony na łodziYoutube
Demony na łodzi
Metafora nieproszonego gościa, bezdomnego Joe
Metafora nieproszonego gościa, bezdomnego JoeYoutube
ACT,gotowość: metafora nieproszonego gościa, bezdomnego Joe
Radio Lęk FM metafora
Radio Lęk FM metaforaYoutube
Radio Lęk FM metafora ACT
Metaphors in Portuguese (Português)
Metaphors in Portuguese (Português) CommunityMetáfora da "Rádio Ansiedade (Anxiety News Radio Metaphor)
Metáfora da "Rádio Ansiedade (Anxiety News Radio Metaphor)The Anxiety News Radio Metaphor described in "Eifert, G. & Forsyth, J. (2005). Acceptance and Commitment Therapy for anxiety disorders. Oakland: New Harbinger.", narrated in Brazilian Portuguese by a specialist in radio ads.
Metaphors in Spanish (Español)
Metaphors in Spanish (Español) CommunityEl invitado indeseado (metáfora)
El invitado indeseado (metáfora)El siguiente es una animación realizada por Joe Oliver utilizando la metáfora del invitado indeseable. Se agregaron subtítulos en español. Es un buen recurso para ilustrar los costos del control emocional. Visite el siguiente vínculo en youtube: http://www.youtube.com/watch?v=z558qPdvYr4
El roble y la espiga: Una metáfora para aprender el concepto de flexibilidad psicológica
El roble y la espiga: Una metáfora para aprender el concepto de flexibilidad psicológicaUn libro ilustrado de acceso libre que adapta la fábula de Esopo: "el roble y la espiga" para ejemplificar la flexibilidad psicológica. La adaptación es de Jorge Everardo Aguilar-Morales y Fabiola Margarita Santiago-García. La ilustración es de Omar Cortés.
Metáfora del barco y la tormenta.
Metáfora del barco y la tormenta.Se trata de una metáfora que he diseñado para abordar los procesos de Aceptación, Compromiso con la acción, Momento Presente y Desesperanza Creativa. Espero que les resulte de utilidad.
"Imaginemos que tu vida transcurre en un barco en altamar, donde usualmente sos el único tripulante a bordo. Conocer la dirección hacia la cual estás navegando resulta motivante y le da sentido a tu viaje, aunque eso no te asegura que el camino sea siempre agradable.
Navegando van a existir diversos factores que no dependen de vos: el viento puede variar, ciertos elementos pueden averiarse temporalmente, a veces será de noche y en algunas ocasiones vas a atravesar fuertes tormentas. ¿Qué sucede en esos momentos en los que los cambios del contexto parecen tomar dominio de la situación?
Muchas veces podemos huir de la tormenta y obsequiarnos la sensación de estar a salvo, aunque esto tenga un precio muy alto a largo plazo: alejarnos del lugar hacia el cual realmente queremos ir. En algunas otras ocasiones, cuando la tormenta es muy grande como para escapar, permanecemos en contacto con aquello que no queremos percibir: podemos dejar de navegar, echar anclas, lamentarnos y preguntarnos por qué el clima es así; podemos discutir con las nubes y el viento, pretendiendo cambiarlas por un ambiente más amable.
Existe una forma un tanto contraintuitiva, a la cual no solemos estar muy acostumbrados: continuar navegando hacia la dirección deseada, aceptando la tormenta tal cual es, sin intentar pelear con ella y sabiendo que, por más aterradora que se vea, es sólo un fenómeno climático normal que se irá en unos momentos, ¡no existen tormentas eternas! En este punto hay una incómoda verdad: a nadie le agrada verse avasallado por una tormenta, no obstante ¿valdría la pena permanecer en contacto con ésta sí gracias a ello te estuvieras acercando hacia donde querés ir?.
Entonces, al encontrarse con una tormenta de la cual no podemos escapar podemos observar dos grandes alternativas: una implica estar en contacto con el malestar de atravesarla, la otra... también, pero con un pequeño detalle agregado: el sufrimiento. El sufrimiento de maldecir hacia las nubes, de pensar en lo injusto que resulta ese cambio climático, de luchar inútilmente por ponerle fin.... el sufrimiento que nos genera el dejar de navegar.
Aquellas ocasiones en las que experimentamos la disposición a continuar navegando sin intentar controlar lo inevitable, podemos contemplar detalles que quizás ignorábamos hasta entonces. Diversas tempestades nos otorgan cierta maestría en el manejo de las velas, nuestra experiencia desarrolla habilidades para atravesar los momentos críticos, podemos conocer las herramientas que tenemos a mano y adquirir dominio sobre su uso. Eso no elimina el malestar generado por el clima, por supuesto, pero nos ayuda a dirigirnos hacia lo que es realmente importante.
¿Cómo querrías actuar la próxima vez que te encuentres atravesando una tormenta?"
Metáfora del tren
Metáfora del trenSe trata de una metáfora de Terapia de Aceptación y Compromiso (ACT) escrita por la Lic. Rocío Arcuri para abordar el pensamiento negativo repetitivo (Pérdida de contacto con el momento presente y Fusión). En ACT recurrimos a este tipo de materiales con el fin de transmitir mensajes terapéuticos y cambiar la forma en la que nos relacionamos con los eventos.
Espero que les resulte útil para la comprensión de estos procesos o como recurso clínico para utilizar con sus pacientes.
Pasajeros en el autobús
Pasajeros en el autobúsPasajeros en el autobús - subtitulos en español
Metaphors in Swedish (Svenska)
Metaphors in Swedish (Svenska)Niklas Törneke (2016). Metaforer - från vetenskap till psykoterapeutiska verktyg. Förlag: Studentlitteratur AB. ISBN: 9789144112244
Metaphors in Turkish (Türkçe)
Metaphors in Turkish (Türkçe)The ACBS Türkiye Chapter has metaphor resources on its website.
Oltaya Takılmak (Getting Caught in the Fishing Line)
Helikopter Görüşü (Helicopter View)
Hayatımın Kileri: Raflara Stoklamak (The Pantry of My Life)
Accept your blood sucking leech
Accept your blood sucking leechMany years ago, a friend of mine had the unfortunate experience of a leech attaching to her leg. Even though it was not easy and a pretty bad scene overall, she allowed the creepy creature to fill itself up and it eventually detached itself from her leg without further incident.
Our first intuition was to rip the leech off; however this could have caused toxic leech vomit to enter her system.
So, the same goes for any unwanted, nasty, and blood-sucking private experiences. While we want to act intuitively and engage in experiential avoidance (which most likely will contribute to the problem worsening later on) we have to learn that sometimes it is just best to OPEN UP to and ACCEPT the situation. Just like a leech, these experiences can be bothersome and painful to observe, but they won't kill you. Just thinking about this now, my friend must have engaged in a huge amount of defusion from leech-related thoughts during those 25 minutes.
Auctioning thoughts/feelings
Auctioning thoughts/feelingsRelatively new to ACT, I thought of this metaphor with clients who have a hard time with anxiety/intrusive thoughts:
Imagine you're at an auction where thoughts/feelings are being auctioned off. You're allowed to inspect the 'products' before the auction begins, observing what they're like, possible functions, even how you might categorize them. When the auction begins, you sit down and "positive" thoughts come up first, then later more difficult thoughts/emotions. Which thoughts/emotions do you want to bid on and how much are you willing to pay for them?
Often, the client will say "I don't want to pay anything for the negative ones", to which I'll reply "well it seems like you're paying a lot for them right now, what might be a reason for you doing that?".
As I said, I'm quite new to ACT so there may be aspects of this that are not precisely ACT-consistent, so any direction on that would be great.
Greetings I'm relatively new - Response submitted by mihail.m.nedkov on January 28, 2017.
Greetings
I'm relatively new to ACT too, but either way I'd like to share my thoughts on the metaphor you've crafted.
In my honest opinion, it's very good at having the person experience in a more evocative way the costs of clutching to certain thoughts. However, I think that this metaphor would suit work on defusion from the conceptualized self better.
Also, I suppose that the part with bidding on positive thoughts might fuel some experiential avoidance - "bid on the positive ones and they'll come more often / will become more believable / will manage to push the negative ones away" and if I were to use this metaphor, I'd drop this part.
Overall, you've created an excellent metaphor which allows for variations - e.g. bidding on eBay / bidding against your valued directions (for example something in the lines of "Do you think the life you'd like to lead / the person you strive to be would be the highest bidder on that thought? Why not?)
Becoming a Lawyer for your Family Traditions
Becoming a Lawyer for your Family TraditionsI have used this with couples and individuals who are hook around 'being right' or taking a position that does not necessarily align with their personal values.
"How has your mind tricked you into taking on the role as a defense lawyer for your family traditions?"
This seems to help people be less 'fused' with historical content they carry with them into relationships outside their family of orgin.
Boat Metaphor
Boat MetaphorThis is a hybrid of the Russ Harris' boat with monsters metaphor and weather as emotions metaphor to explain commitment to values.
You have an indestructible ship that only you can steer. You have serveral compasses on your ship (that represent different values). Because there is nothing that can destroy your ship, and you're the only that can steer it, the only thing that moves your compass needle(s) away from the direction you need to go is you. The weather is your emotions- sometimes choppy, sometimes calm, but they can't actually move the boat. The animals and the sea monsters are your thoughts- sometimes scary, sometimes pleasant, sometimes beautiful, sometimes terrifying, but they can't actually move the boat.
Bumblebees ('the struggle') metaphor
Bumblebees ('the struggle') metaphorBumblebees ('the struggle') Metaphor
By: Alexandra Zax & Dana Bakula
Purpose of the metaphor:
This metaphor was created to help explain the “struggle” we can get caught up in with our mind to individuals across the lifespan (children to adults). This metaphor can help set up talking about how ACT is different from the ways we often think about dealing with stressors. This metaphor was created as an alternate option to metaphors like quicksand and ‘caught in a riptip’ that may be challenging for all children or adults with intellectual disability or cultural differences to relate to.
Metaphor:
Let’s think about our current approach to stress. When we experience stressful, scary, sad, or frustrating thoughts or feelings, our instinct is often to try to get those thoughts and feelings to go away.
For instance, sometimes our instincts tell us to avoid these thoughts and feelings. Our mind wants to focus on something else or maybe try to control everything we can, to keep the scary thoughts from being true. We call this “the struggle.”
This probably works some of the time, which is why we keep doing it! But there are costs to to the struggle. Also, somehow those thoughts and feeling always seem to come back.
To understand the struggle better, let's think about an example. For this example, let’s think about what our normal reaction is around bees. Imagine you are walking outside, and you suddenly find yourself surrounded by a bunch of bees.
Quick! What do your instinct tell you to do? Do you kick? Swat at the bees? Do you run?
If your answer is to struggle (run, swat, kick, flail) then your instincts are the same as the rest of us! But - what happens if you starting swatting at the bees or start running away?
Does that help you?
That’s right – swatting and waving your hands at the bees makes them really angry and scared. That makes them want to sting you. Do you know what actually helps you escape a bunch of bees?
Staying super still and calm like a statue. When you do this, the bees start to calm down and lose interest in you. You are still surrounded by the bees, that has not gone away – but they are no longer angry and you can slowly walk away to safety.
Chessboard
ChessboardThis is a simple presentation of an ACT exercise commonly used in therapy that illustrates the difficulty with getting caught up in one's thoughts, as well as a way to change one's relationship to them.
Compendium of ACT Metaphors
Compendium of ACT MetaphorsAs part of my workshop in Parma on metaphors, I compiled many of the ACT metaphors with example "scripts" of how they are presented in session. Here it is.
Dropping Anchor (Opioid Substitution)
Dropping Anchor (Opioid Substitution)People get into Heroin or Morphine for all kinds of reasons. You can compare it to getting into boating. At first you are given free rides and you like it. Then you get your own boat and you enjoy your trips. But soon you find yourself adrift at sea attacked by pirates. You have to seek shelter in a shark infested archipelago, full of reefs, sandbanks, rocks and dangerous currents and things get really unpleasant and very scary.
The sensible thing to do now is to throw in your anchor (which is a good metaphor for the Methadone substitution program). You are still in the same territory but for now you steadied the boat and you are safe from running aground, drowning and beeing eaten by sharks.
Remember, at that point there is nothing wrong with that sea anchor (Methadone). Lifting it (reducing/stopping) will not by itself be of benefit to you. You are not making any progress by setting yourself adrift again in those dangerous waters. In this situation the anchor is not your problem, it is your salvation.
But over time you will want to move on. So you think about where to go from here, looking for a safe direction and a worthwhile goal.
Once you have made up your mind where you want to go, you plot a course out of the treacherous waters. Now your anchor has turned into a hindrance and lifting it (i.e. getting off the Methadone) will set you free to move towards the goals you have chosen according to your deeply held values.
Makes sense?
I have adapted this metaphor for clients with OSFED, BED & BN - Comment submitted by Maria Aleksandr... on December 8, 2018.
Hi,
I have adapted this metaphor for clients with eating disorders (OSFED, BED, and BN in particular) who doubt whether they have to start working with a dietitian. Here how it goes:
Dropping Anchor (Starting a Meal Plan)
People get into addiction to food and binge eating for all kinds of reasons. You can compare it to getting into boating. At first you are given free rides and you like it. Then you get your own boat and you enjoy your trips. But soon you find yourself adrift at sea attacked by pirates. You have to seek shelter in a shark infested archipelago, full of reefs, sandbanks, rocks and dangerous currents and things get really unpleasant and very scary.
The sensible thing to do now is to throw in your anchor (which is a good metaphor for the Meal Plan. You are still in the same territory but for now you steadied the boat and you are safe from running aground, drowning and being eaten by sharks.
Remember, at that point there is nothing wrong with that sea anchor (Meal Plan). Lifting it (not following/stopping) will not by itself be of benefit to you. You are not making any progress by setting yourself adrift again in those dangerous waters. In this situation the anchor is not your problem, it is your salvation.
But over time you will want to move on. So, you think about where to go from here, looking for a safe direction and a worthwhile goal.
Once you have made up your mind where you want to go, you plot a course out of the treacherous waters. Now your anchor has turned into a hindrance and lifting it (i.e. getting off the Meal Plan) will set you free to move towards the goals you have chosen according to your deeply held values.
Makes sense?
Emotions, the weather and 'We've got cows'
Emotions, the weather and 'We've got cows'Today I had an interesting experience working with a 50+ woman with PTSD/GAD secondary to horrid childhood and marital abuse.
I was using Russ Harris' emotions are like the weather metaphor, including a mindful walk to experience today's weather. While debriefing the exercise we talked about how weather shows up and how futile it is to stand and curse the weather. Actually for her it is not futile - cursing the (real) weather is a form of emotional regulation and mostly soothes her, as long as she then connects with her values and engages with life. Sometimes this engagement means "staying inside" - forsaking some important activities while pursuing other "indoor activities" until the storm passes. But sometimes it means putting on wet weather gear and braving the cold, getting soaked to the bone while doing something more important (for her - feeding the animals).
We then compared this with how she handles the emotional weather. Two of her "storms" were memories and thoughts regarding mother - whom we labelled "Cyclone V...." and her stepfather "Tornado T..." The process of labelling them as such brought instant defusion. Running with the tornado theme, I asked her if she liked the movie Twister and she broke into a big grin and before I could say it she said "We've got cows".
As we explored it a bit further, she realised her experience of anxiety and trauma memories was very much like the scene from Twister - dodging cows, trucks and trees, getting scared out of your wits while pursuing your values.
When I told her I thought she'd invented a new therapeutic technique that might help others as well as herself, she literally glowed.
So she's going away to practice noticing the weather, labelling Cyclone V and Tornado T when they turn up and defusing via "we've got cows".
Ironic that the speaker of the lines was a therapist :-)
What other ways do you fol use the weather metaphor and popular culture?
Feelings are like Geysers
Feelings are like GeysersThis is written with kids in mind to help with Acceptance:
Yellowstone National Park is world-famous for its spectacular geysers, like “Old Faithful”. Geysers are interesting natural wonders. They are hot springs of water which when they get hot enough to boil they send all the water into a tall plume or jet of water into the air. But, they only work like geysers if they have all of the following: heat, water and a plumbing system that clogs up. If they don’t clog up they are just a hot spring of water in the ground. One hot spring in Yellowstone is the Heart Spring, which is a beautiful deep green pool of water shaped like a heart. If they do clog up, pressure builds up and it “blows its top”.
Yellowstone has so many different geysers. Old Faithful erupts every 35 to 120 minutes all day every day for 1 ½ to 5 minutes at a time and the water reaches a height of between 90 and 184 feet in the air. Even though you can count on it erupting, even it is not on a set schedule.
The Giantess Geyser can erupt violently with bursts up to 100 to 200 feet high and the area surrounding may shake from the underground steam explosions. Its eruptions can occur two times an hour for between 4 and 48 hours but only two to six times a year.
Sawmill Geyser erupts and spins water around its crater so it looks like a circular blade of a lumber mill. However its eruptions can last all kinds of different times. It can be between 9 minutes and 4 hours.
They all have something in common: they erupt! Human beings erupt, too… but not exactly like a geyser. We erupt with words or actions “blowing out tops”, too. If we remember what is necessary for geysers to be geysers, it is they “clog up” and build up a lot of pressure. If we try to push a feeling down and try not to think about upsetting things we “clog up” too. If we only think about upsetting things, we can be like the Giantess Geyser with the ground shaking and huge bursts of hot boiling water. We can get out of control.
So, what’s a person to do? Well, noticing our feelings and letting them bubble up like a hot spring doesn’t usually hurt anyone. However, they may be very hot and we have to respect the feelings, just like you can’t do a cannonball dive into a hot springs. You may need to find out a little about the feeling and ease into it and learn all about it.
By the way, Yellowstone National Park has a live webcam of Old Faithful geyser: Old Faithful Geyser Live. Check it out!
Fish in the Water
Fish in the WaterAnother one I've been using regarding the mind and language is the asking a fish if they're wet metaphor. We're the fish, and language is the water. How would a fish know if they were wet if they'd never been out of the water? Jumping out of the water helps you to notice the water, but we all still must swim in it.
Any refinements or thoughts would be helpful.
Thanks,
Joanne Steinwachs
The variant from This Is Water - Comment submitted by josh.mervis on November 8, 2017.
David Foster Wallace has a variant of it that I think is nice for certain clients:
There are these two young fish swimming along, and they happen to meet
an older fish swimming the other way, who nods at them and says,
“Morning, boys, how's the water?” And the two young fish swim on for a
bit, and then eventually one of them looks over at the other and goes,
“What the hell is water?”
If at this moment, you're worried that I plan to present myself here as the
wise old fish explaining what water is to you younger fish, please don't be. I
am not the wise old fish. The immediate point of the fish story is that the
most obvious, ubiquitous, important realities are often the ones that are
the hardest to see and talk about.
Flipping through magazine advertisements
Flipping through magazine advertisementsThis metaphor is used to create defusion. I have client's flip through a magazine and ask them which ads they buy into or they would purchase. I ask what ads to they find helpful or unhelpful. We then make the analogy to how their mind works. Their thoughts are like each ad in the magazine and it is as if their mind is flipping through each page, but they decide which thoughts they want to buy or hold onto.
Flyfishing and getting hooked
Flyfishing and getting hookedI have just been on a four day workshop here in New Zealand with Robyn Wasler – and it has stimulated a number of metaphors.
Here is one that can be used around the idea of ‘buying’ our thoughts/feeling/reactions and treating them as if they are real. It also covers that it is part of the human condition to ‘get hooked’ – but that we do not need to stay hooked if it is our own mind that has hooked us.
Flyfishing Metaphor
“Have you heard about fly fishing. A good fly fisher knows exactly what the trout are feeding on and tie up flies that imitate those insects. They are so good at this that the trout can not tell the difference. They cast the fly into the stream right in front of the trout – the trout sees it floating by – buys that the fly is real, bites and gets hooked.
Our minds can be like really skilled flyfishers. Our thoughts and feeling are like really specific flies our mind designs and are just the ones we will bite on. Our mind casts them out on the stream in front of us – they seem so real to us and so we ‘buy’ them, bite and get hook.
Once we are hooked, the more we struggle the more we are behaving in ways that pulls the hook in further and keeps us on the line.
Funny thing is our mind can only tie flies on barbless hooks. It feels like we can’t get off, but if we pause from the struggle and spit the hook out – we are off the hook. Our mind will tell us there is a barb on the hook and we can’t get off – but if we stop struggling so hard, we get off the hook.
As we swim in the stream of life there are flies floating by on the surface all the time. As we get better at spotting ‘ that is just another fly floating by – I don’t have to bite’ we get hooked less often. But it is part of being human to get hooked on a regular basis. Remembering these flies are always on barbless hooks allows us to spend less time struggling, to get unhook and to then have the flexibility to swim in the direction our values let us know we want to."
Fusion/ Defusion: The Campfire Metaphor
Fusion/ Defusion: The Campfire MetaphorPurpose: This metaphor is used to illustrate the “unworkability” of trying to “fix” (e.g. reduce, remove, suppress or change the form of) difficult “automatic” thoughts and emotions, by “adding” new thoughts when they appear in our “experiential window”. (as when clients try to "solve" these internal experiences with self-debating, or when clients are fused with their thoughts).
This is a heavy tested metaphor, rated as “successful”. Change the words, or explanation procedure, as needed, when using this metaphor on your own.
(Download metaphor as attachment).
Hot Air Balloon Metaphor
Hot Air Balloon MetaphorLessons from the Skies: A Hot Air Balloon Metaphor (shared by Brianna Z. Kauer, M.S., BCBA)
Growing up with a dad who was a hot air balloon pilot meant I had many experiences in the sky. It wasn’t until I was an adult that I realized how out of the ordinary this actually was. For me, it was a normal thing we did every calm summer evening; Soft Skies Balloon Rides was our family business. We spent many evenings preparing for the flight while explaining the mechanics to awed and excited customers who were about to experience it for the first time.
The process became second nature. We began with checking the wind, and then watching the direction of the helium balloons we would send up beforehand, rolling out the balloon in the field next to our house, connecting the basket, listening to the the sound of the fan blowing air into the balloon, checking instruments, velcroing seams together at the top, pulling material, holding ropes and then finally lighting the fire. The burners would ignite, drowning out all other sounds while the balloon went from laying on its side to floating over our heads. Passengers would climb into the basket, the ropes would be released and we would slowly rise off the ground. As the youngest in the family, I didn’t add much weight to the basket which meant I got to go along for many rides.
Floating in the sky above Wisconsin farmland was a big part of my childhood. It was a familiar space and one of the most peaceful places I’ve ever been. Not only did I have many adventures, but it also has given me some insight into perspective taking and letting go.
Many of the people we took for a balloon ride would be surprised to learn that you cannot steer a hot air balloon. The balloon follows the path of the wind and you must go along for the ride. All that you can control is going up or down; adding more heat by lighting up the burners (up) or releasing hot air through the top valve (down).
The balloon ride can be a great metaphor for life. There is so much we cannot control. We cannot control the direction of the wind and if we struggle against it we will only waste our energy. When we allow ourself to surrender to the wind we may notice the things around us in a different way. When we go up or down in the balloon our perspective will change.
The distance from which we look at something impacts our experience.
When we are flying low to the ground, everything seems large and appears to be moving quickly. When you are flying high in the air, everything seems small and appears to be moving slowly. We can’t control which direction the wind blows us, but we can choose to rise above the struggles of the day to see them from a distance. When we create distance from our negative thoughts or feelings they don’t seem so big; mountains become foothills, houses become toys, people become ants.
This distance gives us a bigger picture and often we can see things we couldn’t see before. We might notice other details or possibilities.
What I’m describing is a process called cognitive defusion which is a component of acceptance and commitment therapy and has shown to have a huge benefit on mental health and wellness. The goal is not to escape or avoid those difficult thoughts or feelings, it’s just to see them from a different angle. To create some distance, so that we are looking at them rather than from them.
Many of us learn complex information and concepts best through the use of story and metaphor. Metaphors are especially useful when understanding concepts of cognitive defusion. Finding an exercise or metaphor that works for you can be a useful tool for the difficult moments.
The hot air balloon metaphor is one of many ways to practice this technique of defusion. Other common exercises include observing your thoughts as a train on a track, or leaves on a stream, or playing with the words themselves (de-literalizing language).
When you find yourself overwhelmed by a thought or feeling, you can jump into your hot air balloon basket and float above it. Notice how your perspective changes as you float above those difficult thoughts and feelings. You can go up and down to change your distance from them while you surrender to the path of the wind and see where life takes you.
If you'd like to see pictures of my families ballooning adventures you can see the original post here: https://createbehaviorsolutions.com/lessons-from-the-skies-a-hot-air-balloon-metaphor/
Guided Defusion Exercise (also found here):https://docs.google.com/document/d/e/2PACX-1vQ-UW8WJLjluTLrNI8-emWvu6MlGJ2zlHHb8NeQCaquKvgvNt8eiM9XBJcXreGni7IL-a6jRYFkBilu/pub
Hot Air Balloon Metaphor: Defusion Exercise
You are welcome to close your eyes for this exercise if that helps. If at any time you need to pause, just open your eyes and do what you need to do.
Begin by noticing your body in space. Take a few deep breaths and arrive wherever you are.
We are going to practice putting some distance between you and your thoughts and feelings.
We will start by imagining yourself climbing into a hot air balloon basket. You look up and see the fully inflated balloon over your head filled with warm air.
Outside of the basket on the ground are all the things that have been troubling you. It is hard to see anything else because they are taking up so much space around you and are very big. Picture your troubling thoughts and feelings as actual objects on the ground. They could take shape as houses, vehicles, people, books, animals, to do lists, cell phones, or maybe just abstract shapes or different colors.
When you are ready to take flight you reach up and pull the burner which blows fire and heats the air of the balloon. That air begins warming up and soon the balloon gently rises off the ground and into the air.
You feel weightless and free.
You continue to rise.
You can feel the breath moving in and out of your lungs naturally with ease.
If you notice yourself getting closer to the ground you can simply add more heat to the balloon to rise higher into the air.
As you float upwards, you look down to see the ground and all the thoughts and feelings it holds. Notice how the size of those things looks much different from up here. They are still down there but they are taking up much less space in your line of sight. Now you can see them along with the whole city/town and horizon. You know they are there but from up here you can notice them from a distance.
From up here they are not the only thing you are experiencing.
From up here you can notice your body and the gentle rise and fall of your breath.
From up here you can notice your feet touching the basket.
From up here you can notice the sounds of the birds and the warmth of the air on your face.
From up here you can let go of your agenda and surrender to the direction of the wind.
This space is available to you whenever you choose to come.
For now we will let this image dissolve and bring your attention back to your body in space.
Taking a few more deep breaths before opening your eyes and returning here and now.
Intro to metaphors in ACT
Intro to metaphors in ACTAttached is a ppt & handout I did as an assignment during my final year undergraduate psych study. There's also a video role play of the chessboard metaphor which I've posted on YouTube (search by title "chessboard metaphor"). These materials were designed to briefly introduce other students (with no knowledge of ACT or RFT) to the use of metaphor in ACT as a psychotherapeutic technique. I've used material from this website extensively and hope I've acknowledged those sources adequately. I am sooooo grateful for the wealth of material that is available here!
Life as a cycling race
Life as a cycling raceIn a way, life is like a cycling race. We are all pedaling and we wear shirts with words written on them. In French we have a way of speaking («Vous roulez pour qui ?) that translates litterally into "for whom do you travel ?" The idea is the same as the one Bob Dylan expresses in the song "You've got to serve somebody". We sometimes believe it's possible to have blank shirts without anything written on them or we can "not know" for what we pedal but in this case it happens that we nevertheless have something written on our shirt, namely "NOTHING" or "I DON'T KNOW". And how does that feel to travel for that master?
Now imagine there is a shop with piles of shirts wearing all kinds of words written on them. Like ELEGANCE, GENEROSITY, LOYALTY, HEALTH, LOVE, CARING, HONESTY, and so on. And you can choose, for free, any one of them. Which one would you choose?
And look what happens (at least to me). There comes this voice (you've probably heard it before) that says : "Waah, ELEGANCE, are you kidding? Have you looked at yourself in a mirror? That one for sure is not for you." Or something like "How come you want to take CARING? With that crappy introverted personality of yours? Or like "XYZ, are you crazy? You really don't have the temperament to do that!"
Can you have all these thoughts AND take the shirt you find «way cool», the one showing the quality you choose to «make important» in your life (thanks to Hank Robb for those wordings)? Then, find a goal, preferably a small one, an action that would lead your life a tiny little bit in the direction of that value, and DO it! Of course the voice will come with you, all along the way. See if you can welcome it without trying to have it shut up but without obeying it.
Life direction metaphor
Life direction metaphorA boat docked in a tiny Mexican village. An American tourist complimented the Mexican fisherman on the quality of his fish and asked how long it took him to catch them.
"Not very long," answered the Mexican.
"But then, why didn't you stay out longer and catch more?" asked the American.
The Mexican explained that his small catch was sufficient to meet his needs and those of his family.
The American asked, "But what do you do with the rest of your time?"
"I sleep late, fish a little, play with my children, and take a siesta with my wife. In the evenings, I go into the village to see my friends, have a few drinks, play the guitar, and sing a few songs. . I have a full life."
The American interrupted, "I have an MBA from Harvard and I can help you!. You should start by fishing longer every day. You can then sell the extra fish you catch. With the extra revenue, you can buy a bigger boat. With the extra money the larger boat will bring, you can buy a second one and a third one and so on until you have an entire fleet of trawlers. Instead of selling your fish to a middle man, you can negotiate directly with the processing plants and maybe even open your own plant. You can then leave this little village and move to Mexico City, Los Angeles, or even New York City! From there you can direct your huge enterprise."
"How long would that take?" asked the Mexican.
"Twenty, perhaps twenty-five years," replied the American.
"And after that?"
"Afterwards? That's when it gets really interesting," answered the American, laughing. "When your business gets really big, you can start selling stocks and make millions!"
"Millions? Really? And after that?"
"After that you'll be able to retire, live in a tiny village near the coast, sleep late, play with your children, catch a few fish, take a siesta with your wife and spend your evenings drinking and enjoying your friends."
Life's a beach - struggling in the rip
Life's a beach - struggling in the ripI've mainly used the "caught in a rip" metaphor as a graphic way of capturing the essence of giving up the struggle. As I've written it down I think it actually has value for many aspects of ACT. So please feel free to email me with ideas for extensions or ammnedments.
Life’s a beach
Sometimes life is like swimming at the beach. We launch headlong into life expecting to have a fun, relaxing and refreshing time. People ply us with good advice. Don’t forget the sunscreen. Swim between the flags. Stay out of the water for 30 minutes after eating. Watch out for sharks. So we jump in, splash around and have a good time. Depending on our personality and experience we may be carefree, or we might be anxiously watching for sharks, or continually monitoring the flags to make sure we’re in the right place. Or maybe we are the sort of person who loves to flout the rules and swims anywhere.
Suddenly our pleasure is interrupted by an unpleasant sensation. We are knocked off our feet, we can no longer touch the sandy bottom and we notice we are headed out to sea. We panic and immediately set the goal, “I must get back to shore” so we take action to achieve that goal. We do it without thinking. It’s instinctive. We start paddling furiously against the rip. Sometimes we seem to be making a little progress, but we start to tire and notice we are losing the battle. We swim harder, we roll over on our back and kick with our legs, but we are getting nowhere and getting exhausted. We forget why we came to the beach in the first place. We begin to tell ourselves, “If only we had stayed between the flags” or “I wish I’d done some more swimming training before I risked it all by coming to the beach”, but none of this wondering how you got here is any help. You are still paddling furiously and getting nowhere. Maybe you call for help, and here I am – a lifesaver come to the rescue. So notice – here I am with a board to rescue you, and I suggest you grab hold of the board. Before you can grab hold of the board you need to stop paddling furiously. Even though every fibre in your body screams in protest, you must stop paddling and try something different – grab the board.
Now I am a very contrary lifesaver, for my job is not to rescue you, but to teach you to rescue yourself. For the thing about life is you can get sucked into a rip at any time. That rip may be depression, or grief, or anxiety or urges to eat, gamble, spend or use drugs.
So I want you to learn how to get out of trouble when you get stuck in a rip. So I invite you to swim slowly across the rip. I’ll even swim alongside you. As you do this you will feel the tug of the rip. You will get carried out to sea further than you’d like to be and your mind will flash all sorts of scary scenarios before your eyes. That is what minds do. Mine does it too. I’m not asking you not to be scared, or anxious, or depressed. I’m asking you to swim across the rip while experiencing those thoughts and sensations and eventually you will come to calm water and be able to get on with enjoying your day at the beach. So what I’m inviting you to do is to give up paddling furiously and accept the uncomfortable sensations and scary thoughts of being carried out to sea. I’m inviting you to reconnect with what really matters – having fun at the beach for whatever reasons that is enjoyable for you. I’m inviting you to take effective action and what that is depends on the situation. If you’re safe it means enjoying the sun and the surf for your own reasons. If you’re stuck in a rip of (insert presenting problem) it means stopping the struggle and taking small strokes in the direction of where you want to be, whatever experiences come up.
Additional Extensions
(For OCD/Anxiety)
Notice that in this scenario there are precautions you can take to improve your safety. You can learn skills like how to do survival stroke, or simply train to be a better swimmer. You can put on sunblock to stop getting burnt. You can stay out of the surf on really rough days. You can avoid beaches where there are stingers. You can swim between the flags. These can serve to improve your enjoyment of being at the beach. But what happens to your fun if you become obsessed with safety. Instead of floating around or catching waves, you keep your eyes glued on the flags? Or as soon as your toes hit the water you run back to your bag to put on some more sunblock? Or if you give up on going to the beach because it’s too dangerous? (Let client answer – and discuss reasonable safety and how to practice it as well as willingness to have worry thoughts while pursuing valued activity)
Notice also that despite your best efforts, you can still get stuck in a rip. Winds, current and tide may change and the area that was once safe turns into a rip, or maybe a huge wave comes and knocks you off your feet. It doesn’t matter whose fault it was or how it happened, once you’re in a rip you have an important choice to make. Keep struggling and eventually succumb to exhaustion and drown, or stop struggling and start taking effective action by swimming across the rip towards your values.
(Values)
Notice that there are lots of people at the beach on a hot day. Now I imagine they’re not all there for the same reason. What are some of the reasons for going to the beach? (Let client answer and prompt for as wide a range of options.) Use this as a jumping off point for discussing goals and values including pursuing the same goal for different reasons, and also being able to pursue values even if a specific goal is blocked. For example if you go to the beach (goal) to cool down (value) – if the road to the beach is closed, there are other ways to cool down – e.g. – sit in an air conditioned room, have a cold shower, have an iced coffee etc.
(Advice/Pliance/Programming)
Do you remember all the good advice people have given you about how to be safe when going to the beach? Notice that some of it is good advice (don’t get out of your depth if you can’t swim), some is mostly right but sometimes wrong (it’s safe to swim between the flags) and some is just urban myth (rubbing butter on your skin protects you from sunburn). I’ll bet you didn’t ask for any of that advice, it just randomly came your way. People with good (and maybe bad) intentions filled your head with a mixture of good, bad and indifferent advice. So how do you tell whether that bit of advice that pops into your head when you make plans to go to the beach is worth following? (explore workability)
Mailbox metaphor (some thoughts are like junk mail)
Mailbox metaphor (some thoughts are like junk mail)I use this with clients who are experiencing troubling thoughts. I find it helpful as a rapid analogy about value driven behavior and acceptance. In addition, the metaphor itself is easily anchored , as most of us actually check a mailbox each day. I enjoy sharing on this site, feel free to play with this , and offer your feedback.
1) When you go home today, what do you expect to find in your mailbox?
Client answers: Bills, advertisements, junk mail, maybe a letter.
2) How do you sort through to decide which mail needs follow up and which is considered junk?
Client answers: I have to look at it, and decide what is important.
3) How do you know what is important?
Client: Well if I don’t pay my bills my electricity would get disconnected, and if I don't renew my license plates, I can't drive.
4) I see, so you sort things out according to what matters to you, your priorities are easy to identify because you value the stability of a comfortable home and the freedom of driving your own vehicle. What do you do with the junk mail?
Client: I throw it away
5) When you throw it away, is that the end of it?
Client: no there's always more junk mail the next time I open the box.
6) Why don't you follow up on it? You could call and check on those offers or you could get mad and call the advertisers and demand that they stop delivering the junk?
Client: Yes, but that would just be a waste of time…I've learned those offers are things that I don't need, or they are scams. I once tried to stop the mail but other companies send more. There's always more junk mail the next day, it's not worth getting upset..
Summation: So your experience helps you sort out what is important, according to the things that matter to you. And you learn to live with the junk mail that shows up everyday. It's in the box, you notice it long enough to recognize it for what it is, and then you move onto what matters in your life. …… Maybe these thoughts are like the mail that shows up in your mailbox; you take action on the important things while you have to accept the fact that there will be some junk , and you simply allow it to show up.
Mindfulness body based ACT metaphors
Mindfulness body based ACT metaphorsThis is a file with several mindfulness body based ACT metaphors that consist in guided mindfulness of the body exercises that target specific processes specially shifting mode of mind from doing mode to being mode. They all enphatize learning from direct experience and connecting with here and now. You can explore more you can go to the ppt presentation at WC IX for more resources. Hope you all enjoy them! and if you use them please let me know how was your experience.
embodied metaphors for couples work
embodied metaphors for couples workThis are the handouts of the metaphors used in the WC13 in the "When it takes two for acting mindfully workshop".
embodied metaphors from Dublin conference
embodied metaphors from Dublin conferenceThis are the embodied metaphors presented in the workshop at Dublin
Mosquitos with megaphones: acceptance vs. experiential avoidance
Mosquitos with megaphones: acceptance vs. experiential avoidanceThis is a metaphor I'm working on to help explain the utility of acceptance. I'd really love to get feedback if folks have any thoughts. --Melissa Wright
Therapist: Sometimes it seems almost impossible to sit with our feelings. I’d like you to imagine something that might help you understand what I mean about “making room” for your experiences, or accepting them. Would that be alright?
Now imagine you are walking home your usual way, just walking through your neighborhood. Suddenly, you hear something, and it sounds like it’s right behind you. It sounds big, it sounds scary, it actually sounds like a giant flying beast… you think you can hear its massive wings flapping and its jaws crunching and grinding. Terrifying sounds. My guess is you might take off running, does that sound about right?
Client: Well yeah.
Therapist: Me too. Are you a runner?
Client: Oh, sometimes. I’ve been a runner in the past.
Therapist: So, tell me… what happens once you’ve been running for a mile or so?
Client: Well I should be fine after a mile.
Therapist: Okay, so what about after five miles?
Client: I’d definitely be getting tired by then.
Therapist: I certainly would too. And what do you normally do while you’re running?
Client: What do I do?
Therapist: Yeah, I mean, do you make business calls, or catch up with the people you love?
Client: While I’m running?
Therapist: Yeah, while you’re running.
Client: Well, no, running is pretty much the only thing I do while I’m running. I mean I get all sweaty and out of breath.
Therapist: I’d certainly be sweaty and tired. But the thing is, the beast is still following you, so you keep running. You run and run and run and run and you are sweaty and you are tired, but the beast is still there, you can hear it, so you keep running.
Finally, at some point, you trip over a rock. And when you look up, you see it. And this beast that’s been following you? … Now, bear with me, this is a funny image, but this beast - well… It’s a gang of mosquitos. There’s about 8 of them, and they are flying around with these little megaphones that make them sound MUCH bigger than they really are. And those big wings that you thought you could hear flapping? They are actually tiny mosquito wings… and those jaws that were grinding? That’s actually the noise of the tiny little mosquito mouths…
But you’ve stopped running, so now they do bite you. And you sure do get itchy. And that’s actually pretty unpleasant… but do you think that at this point, as you’re looking up at the mosquitos, you would choose to get up and start running again?
Client: I guess not, if they are just mosquitos…but what do you mean?
Therapist: Well, sometimes running does make sense, right? If its really a monster you need to avoid, then running makes sense. But the thing is, feelings are a lot more like a pack of mosquitos chasing you around than an actual monster. No one has ever been injured or killed by anxiety and sadness. Feelings ARE itchy: they often aren’t fun, they can be downright awful to experience. But if we run from them, we end up using all our energy getting sweaty and out of breath, while we could have been making business calls, catching up with old friends…
Client: Hmmm
Therapist: The important thing to remember is that even when feelings and thoughts look and sound like a huge crazy monster, the truth is, they can’t actually hurt you.
And what I’m hoping is that, above all, we can help you notice when you are running. That way you can make a decision -- you can ask yourself, “is running actually helping me get what I want? Or, am I all sweaty and tired and unavailable to my friends and family because I’m so busy running away from something that isn’t actually dangerous to me?”
Running takes a lot of energy, and you might find that you’d rather get a few mosquito bites, feel the itchy feelings, and be able to stay in one place and do the things that you want to do. But it takes practice to know that you’re running, practice to learn how to keep walking instead, and I’m hoping we can practice some of that here together.
New animation of the Chessboard metaphor
New animation of the Chessboard metaphorInternal Struggles (The Chessboard Metaphor) - Contributed and posted with permission by Dr. Russ Harris
Here's a brand new animation of the chessboard metaphor. It is posted on YouTube so you can freely share with clients if you wish.
Passengers on a Bus
Passengers on a BusPassengers on a Bus - An ACT Metaphor: https://www.youtube.com/watch?v=Z29ptSuoWRc
Les Passagers du Bus (Français): A French animated Choose Your Own Adventure video series featuring The Passengers On The Bus metaphor. Viewers are able to make decisions that shape the story, with each video demonstrating the impact of their chosen strategy: https://www.youtube.com/watch?v=TYjIYp-46zc
Illustrations for ACT Willingness and Passengers on the Bus Metaphors
Illustrations for ACT Willingness and Passengers on the Bus MetaphorsAttached are two illustrations that may aid in conveying Willingness and the Passengers on the Bus metaphor to clients. Design credit to Michael Kremer, Art credit to Pat Kremer.
Room full of adhesive tape
Room full of adhesive tapePicture your life as a room. One day you notice that a pipe near the ceiling in a corner is dripping. The sound of the falling drops makes you nervous and you'd like to get rid of it. So you repair the leak with a length of adhesive isolation tape and your peace of mind is back. Until the water finds his way through the glue and the dripping sound is back. Plop.... plop... plop... So you put one more length of tape around the first repair and you are quiet again. Of course your quietness doesn't last very long and you have to fix the leak again and again. That's not a great problem since adhesive tape is pretty cheap and you manage to always have a spare roll handy. It can take months, even years until you notice that that big clumsy repair slowly fills the whole room, that there's less and less space for you to live in and that the dripping comes nearer and nearer to you...
This metaphor adresses basically the same problem than the «feeding the tiger» metaphor. The hopelessness it conveys seems to me to be more «creative» since it doesn't lead to the thought «it's too late now, the tiger has grown so huge I really can't do nothing else than feeding him» clients will often buy when the «feeding the tiger» metaphor is presented.
Sandstorm metaphor to illustrate ACT processes
Sandstorm metaphor to illustrate ACT processesSandstorm metaphor
Sandstorms are violent wind storms that occur in the desert when high winds lift particles of sand into the air thus unleashing a turbulent and suffocating cloud of sand. They can occur unexpectedly and last for as little as a few minutes or as long as a few months. Regardless of how long they last, the effects can be abrasive and blinding to exposed skin. To survive a sandstorm one therefore has to experience the sandstorm from a different position of having exposed skin covered, and ‘riding’ the storm. A sandstorm can move whole sand dunes, thus changing the landscape. It can therefore be difficult to rely on the landscape to show you which direction to go in. The stars which are constant and remain unchanging can be used instead as a compass for guidance. There is therefore a real danger of getting lost in a whirling wall of sand, as well as the abrasive effects on exposed skin and eyes. To survive a sandstorm, one has to cover exposed skin, and then sit and wait for it to pass whilst experiencing the sights, sounds, smell, taste of the storm, but doing so from a position that allows you to experience it, but not be caught up and exposed in it. Major sandstorms are a natural occurrence – they are part of life in the desert and cannot be avoided.
Difficult life situations/worries/anxieties/fears/problems can be like sandstorms. They are a natural occurrence of life and living. We can sometimes feel as though we are caught in the middle of a sandstorm, lost (moving sand dunes and changing landscapes), and unsure of which direction to move in.
The enclosed attachment illustrates two ways of responding when caught in a sandstorm - psychological flexibility and psychological inflexibility, and the different ACT processes within each.
Standing on the edge of a cliff metaphor
Standing on the edge of a cliff metaphorI recently used this metaphor with a lady with needle phobia that regularly needed to be cannulated to receive cancer treatment. She hated the experience and had the urge to rip the needle out of her arm. Having the treatment was in line with her values as she wanted to live.
‘Have you ever stood on the edge of a cliff or the balcony of a high rise building when you’ve suddenly had the thought ‘what if I jump’? (most people have had that experience and she said ‘yes’). How did you feel? Did you ever think that you would actually jump? Did you know that you were in control over whether you jumped or not? Must people experience a surge of anxiety but know that they would never jump.
What if it’s the same when the needle is put in your arm and you are attached to the drip?
You can’t control the thought (what if I jumped/pulled the cannula out of my arm?), but you have a choice to jump or to stand back and admire the view?
This lady felt much calmer in the subsequent cancer treatment sessions and said that she was able to sit back and observe her thoughts rather than buying them.
Although I used this with a lady with needle phobia it could easily be used with any situation where the client fuse with a thought and believe that they might act on it.
Steve's Battlefield Metaphor (excerpted from forum)
Steve's Battlefield Metaphor (excerpted from forum)Plain language version of ACT Submitted by Steven Hayes
This is ACT in a few sentences: You've been trying to win the war with your mind, with your anxiety, with your urges [add whatever is relevant]. True? (They always say "yes."). Well, ACT is about letting the war roll on while you leave the battlefield.
The "Shredding Paper" Joke (Workability)
The "Shredding Paper" Joke (Workability)This is a joke I've been using with clients recently that seems to have been pretty successful so far in orienting them to the concept of "workability."
There's this little boy that won't stop shredding paper. No matter what his parents do, every piece of paper they put in front of him, he tears up. They take him to three different doctors to see what they can do to fix it. The first doctor says that his problem is psychological, and so he prescribes him six sessions with a therapist. At the end of the sessions, they put a piece of paper in front of the boy...and he shreds it immediately. The second doctor says his problem must be neurological, so he does a bunch of tests and prescribes a bunch of different medications in an attempt to curb the behavior, all to no avail. So they take the boy, who by this point is incredibly frustrated by this entire process, to see a third doctor. This doctor, rather than writing a prescription or doing some kind of complex diagnostic, simply walks up to the boy, bends down and whispers something in his ear. The boy looks at him, says "Okay!" and from that moment on, the behavior completely stops. A few weeks go by, and it looks like whatever doctor number three did fixed it. So, curious, the boy's parents ask him what incredible piece of wisdom and insight the doctor gave him. The boy replies:
"He told me if I stopped shredding paper then you guys would stop taking me to see these all these doctors."
The Clutch
The ClutchThis metaphor is useful for car enthusiasts, or anyone really, as long as they understand the concept of a clutch in a manual transmission vehicle.
It's as if you're driving a car on your journey through life. However, you begin to notice over time that the engine in this car is very finicky, almost like it has a mind of its own. It occasionally revs up very high, or bogs down low. As it does this, the car speeds up or slows to a crawl, regardless of the speed limit, upcoming turns, or what the traffic is like around you. Naturally, this can make it difficult for you to effectively drive in the direction you want to go. Your initial response is to try to control the pace of the engine by hitting the brakes when it speeds up or hitting the gas when it slows down. You push down hard on the brake, and you slam the gas pedal in response to the engine acting up. However, you notice over time that this does not work very well or for very long, and the engine revs even higher or bogs down even lower when you try to fight it. What's more is while you have been putting all of your energy into those pedals, your attention is no longer on the road or the direction you are headed. What if there were an alternative to the gas and brake pedals. What if you looked down to find that there was a clutch, hidden over in a dark area of the floorboard? Instead of trying to control this finicky, unpredictable engine, you could simply take the car out of gear. This would eliminate the need to control or change the pace of the engine, and instead as it begins to race or bog down, you could simply push in the clutch. When the pace of the engine is appropriate or effective for the road that you are on, you could let the clutch back out. The engine no longer controls the speed of the car. You do. And you are now free to concentrate on the road ahead of you. We can think of our minds as being like the engine in this example, and willingness, acceptance, and mindful awareness are all like the clutch. When our mind begins racing, telling us to run away or escape, showing us images of possible dangerous scenarios, reminding us of painful past events, or bogging us down with evaluations, judgments, and negative predictions, we can choose to engage the clutch and willingly observe these things without allowing our behavior (the car itself) to automatically speed up or slow down. When we find that our mind is being helpful, we can release the clutch and allow it to do its work. We can't ever successfully gain control of the engine, but we can gain control of the speed and direction of the car.
The Cold Shower - Willingness/Making room for discomfort
The Cold Shower - Willingness/Making room for discomfortThe Cold Shower metaphor
Taking a cold shower – dealing with discomfort in the service of a valued life. Noticing Willingness and Unwillingness and how to make Willingness easier.
Two scenarios:
You are thinking of taking a shower but you discover there is no hot water:
1. If you had the choice to have a cold shower…or not to, you might choose not to. Because it’s cold, it’d be uncomfortable, you could do without the shower, I will be cold afterwards, I’m not that smelly I’ll do till the morning etc. You might not be bothered because there’s no point in putting up with that much discomfort for no good reason.
2. If a close relative or friend was getting married that day, you wanted to be clean and fresh but again you find there is no hot water. If you stopped for a few minutes and you thought about the person getting married and how much you care about them, and the great time you were going to have sharing in that special day, wouldn’t you put up with a few minutes of discomfort of the cold shower? Because it was Important to You. Mightn’t you be able to put aside your feelings of discomfort, because you wanted to be fresh and clean for the great day ahead? In this instance, we are prepared to make room for the uncomfortableness. We chose discomfort in the value of feeling better after the shower.
In both scenarios, the water is the same unpleasant temperature.
Which of the 2 scenarios would ‘feel’ better? And why?
When we increase Willingness to make room for uncomfortableness it can increase our bandwidth to be able to take on experiences we might previously have avoided.
In the second scenario, I made room for the uncomfortableness and I let it be there, and I still went ahead and had the shower because it was important to me. In the first scenario, I only focused on the uncomfortable feelings and I preferred to avoid the shower altogether.
Finding out what’s important to us in life can really help manage uncomfortable feelings and make room for them by focusing on What’s Important in our lives.
So if someone was socially anxious, yet they wanted to go to a gathering. They could choose to make room for some uncomfortable feelings (to have the cold shower as it were) because What’s Important is that I move forward towards things I enjoy, What’s Important to me, like socialising with others.
The Hockey Goalie: A Metaphor for Psychological Flexibility
The Hockey Goalie: A Metaphor for Psychological Flexibility CommunityThe Jigsaw Piece Metaphor (acceptance, defusion)
The Jigsaw Piece Metaphor (acceptance, defusion)This is a metaphor and defusion technique devised by one of my clients and shared with her permission.
It provides a very simple and powerful image for the acceptance of thoughts which are disturbing and unwanted.
The Jigsaw Piece
When an unwanted or distressing thought arises, I try seeing it on a jigsaw piece.
My jigsaw has many pieces, each representing the many different aspects of myself and my experience.
I see the jigsaw piece with my thought (or feeling) on it as it finds its alloted place in my jigsaw.
There is a space for this piece. It is a perfect fit. It belongs here, for whatever reason, even if I don't understand or want it.
It is a part of my experience. Just that. Even if this piece looks ugly or painful or disturbing, it is one piece of a large and beautiful picture.
As I'm typing this, I'm also thinking of those photo montages where, for example, the picture looks like a face and when you zoom in it is constructed from thousands and thousands of unrelated smaller images.
There is some scope to elabourate this image a little or use it in conjunction with other exercises - for example I sometimes use an exercise called "Big I, little i's" (constructing a big I on the wall using lots of post-it notes, the client being invited to write about different aspects of themselves on each one)...the point being that I am more than any one aspect of myself e.g. I'm more than my appearance; more than my history; more than my intrusive thoughts...
I hope this is helpful.
Regards
Andrew Chester
Sheffield, UK.
The Magical Bank metaphor
The Magical Bank metaphor$86,400 -- Something To Think About!
Imagine that you had won the following prize in a contest: Each morning your bank would deposit $86,400.00 in your private account for your use.
However, this prize has rules, just as any game has certain rules.
The first set of rules: Everything that you didn't spend during each day would be taken away from you.
You may not simply transfer money into some other account.
You may only spend it.
Each morning upon awakening, the bank opens your account with another $86,400.00 for that day.
The second set of rules: The bank can end the game without warning; at any time it can say, Its over, the game is over!
It can close the account and you will not receive a new one.
What would you personally do?
You would buy anything and everything you wanted, right?
Not only for yourself, but for all people you love, right?
Even for people you don't know, because you couldn't possibly spend it all on yourself, right?
You would try to spend every cent, and use it all, right?
ACTUALLY, this GAME is REALITY!
Each of us is in possession of such a magical bank.
We just can't seem to see it.
The MAGICAL BANK is TIME!
Each morning we awaken to receive 86,400 seconds as a gift of life, and when we go to sleep at night, any remaining time is NOT credited to us.
What we haven't lived up that day is forever lost.
Yesterday is forever gone.
Each morning the account is refilled, but the bank can dissolve your account at any time....WITHOUT WARNING.
SO, what will YOU do with your 86,400 seconds?
Aren't they worth so much more than the same amount in dollars?
Think about that, and always think of this: Enjoy every second of your life, because time races by so much quicker than you think.
The Pendulum Metaphor (willingness)
The Pendulum Metaphor (willingness)I'm not too satisfied whith the two scales metaphor. The two scales are unrelated and therefor difficult to understand.
I propose the pendulum metaphor as an alternative. You have two dimensions of a pendulum: one is the amplitude the other is the string between its sinker and attachment. They are clearly related and the metaphor is easy to understand since almost everyone have some experience of a pendulum.
The pendulum metaphor below. It's a remake of the two scales metaphore.
Comments welcome. Feel free to use.

Detta verk är licensierat under en Creative Commons Erkännande 3.0 Unported Licens.
A Pendulum
Imagine a feeling, any feeling or emotion. How long will it last?
Imagine a pendulum. The higher you lift it in one direction, the more power to swing up on the other side will you give it. You will perhaps notice the power in it’s weight and resistance, more when you let it go.
It is with feelings as with the pendulum – they swing! Inexorable! You may like one side more than the other. If you try to fight the pendulum and try to get it high up on the side you prefer, you will give it power to get high on the opposite side (the one you dislike). You may for a short moment stop it or lift it higher then it’s natural cycle (provide). It will though consume and lock your own power. And sooner or later it will anyway go to the side you dislike – and with the extra power you’ve been giving it! Fact is that in the moment you notice a resistence in your strive to get the pendulum in your disired direction, it’s power is in the opposit direction.
If you on the other hand are willing to let the pendulum swing, you don’t lock your energy in the pendulum and you do not give the side you dislike any extra energy. For some persons it may swing more than for others. Some might like it, others are getting seasick. Willingness is not equal to like it when it swing. Willingness is to change focus. Instead of sitting in the sinker, it is to climb up the string to the attachment! It means you have acceptance for all feelings.
At the attachment of the pendulm can you let it swing without getting seasick. The whole of you are not swayed by the swing, but the swing is still there.
Let’s take anxiety as an example:
It is when you are really unwilling to have anxiety that anxiety is something to be really worried about. It is as when anxiety is high and willingness low the anxiety clings hard. And how hard you press the pendulum the harder the anxiety clings. You give it more power. So what is favourable to do is to shift focus from the power of the anxiety in the pendulum to acceptance and willingness. Climb from the sinker to the attachment of the pendulum. You have, in vain, tried for so long to control your anxiety. You can not change the swing (at least not from the position in the sinker) but you are free to climb to the attachment.
That is not a reaction, not a feeling, emotion or thought – is is a choice.
You have probably been at the sinker – you might have been in high swing. That might be the reason you are here. What needs to be done now is to climb up to the willingness in the attachment point of the pendulum.
In doing so, sitting at the attachment wherer willingness is high, I can guarantee you what will happen to your anxiety. I’ll tell you exaclty what will happen, and you can hold an me as a solemn promise. If you stop trying to control anxiety it will be low – or high.
I swear. And when it is low it is low until it is not low any longer. When it is high is will be high untill it becomes low again. I’m not teasing you. There just aren’t enough words for what it is like to sit at the attachment of the pendulum compared to sitting at the sinker.
These strange words are as close as I can get. I can say one thing for sure, and I guess your experience says the same thing – if you want to know for certain where you have the anxiety, there is something you can do. You only need to glide down to the sinker (were willingness is low) and follow it. And sooner or later, when it swings up the anxiety side you don’t want to be there any longer. Then you go in clinch with the pendulum and give anxiety power. It’s very predictable.
If you on the other hand again climb to the attachment where you willingly can let the pendulum swing – you can let it swing both ways! Sometimes there is anxiety, sometimes not. And in both cases you will keep out of a useless and traumatic struggle that can lead only in one direction. Sitting at the attachment of the pendulum and willingly letting it swing without an urge to control the swing (you are not getting seasick and you don’t favour one side) the unnatural unease dissapear and only the natural unease remain.
You can’t say how long it will linger, but one thing is certain - I don’t say the unease will disappear, what I say is that if you give in your attempts to manipulate your unease the degree of unease will be set by your temporary, personal history. No more, no less.
Control works in some areas of life. But not in getting rid of heavy feelings or thoughts. Acceptance and willingness on the other hand work, it’s in your hand. There is a little trap here. There is a paradox. Imagine the rule we mentioned earlier is true: " If you are not willing to have it, you have it."
What can you do with that knowledge? If you are willing to have it – for to not have it – then you really don’t want it.
Are you then willing?! You can not fool yourself.
Simple Simon Metaphor (Defusion)
Simple Simon Metaphor (Defusion)This metaphor is similar to “I can’t walk”, demonstrating that you can choose to act contrary to what your mind is telling you.
All it takes is a quick game of “Simple Simon”: Demonstrate actions preceded by “Simple Simon says do this” and the client follows by doing the same action. When you, however, say “Do this”, the client does not follow suit.
I have used it successfully in training where of course it is a lot more fun, because participants who inadvertently do the action on the command “Do this” are out and the object of the game then would be to see who can outlast everyone else. What I like about this metaphor more than “I can’t walk” is that it so clearly demonstrates the urge to act on the command, yet the ability to ‘urge surf’ to borrow the term from Russ Harris.
Comments welcome, particularly if you have great ideas of how to make it more fun on a one-on-one basis!
Esthe Davis
The Pickup Artist ...
The Pickup Artist ...Am a life coach and new to ACT. (new to life coaching too actually) so I hope others can improve on this metaphor I used with a client and it blew her mind. This is aimed at defusion of nasty thoughts about self. Creating some distance by putting the nasty thought in the mouth of a character you know the clients will hold with some aversion.
So the thought that was expressed by the client was "that's the last thing I am is a genius". I asked her, so if I just thought of something that might sound a little strange at first but might give you an interesting perspective would you want me to share it with you? "Sure" (somewhat guardedly).
So lets pretend you are in a bar. Is there a bar you go to frequently? O.K., picture that one. And you are waiting for a friend. She texts you and tells you that she is stuck in traffic but still coming. While you are waiting, a guy starts to notice you. You ignore but are aware that you are being noticed. After a while he comes up to you and says "Hello my name is Clod". You say nothing and just look at him. Clod says, "I have been noticing you and just wanted to say, the last thing in the world you are is a genius."
What would you do? "Tell him to get lost". Right. That makes sense. What a 'Clod'. But just for fun, what options would you have in that situation? "Well I'm certainly not going to talk to him." Agreed, that makes total sense. But let's just list out the options....Discussion leads to, 1) You could talk to him. 2) You could ask the manager to kick him out of the bar. 3) Ignore him and hope he goes away. 4) Throw a drink on him. I then raised, well tell me if I'm wrong but it sounds to me like you didn't do any of those things. It sounds like you went and sat down with him asked him if you could wear his school ring around your neck. "Huh?" Yes I mean here we were talking about something I thought was ingenius and you told me the last thing you were was a genius, sounds like you are buying into Clod pretty intensely.
In my session it did not result in a committed action step but it could be pursued, e.g. How do you want to respond to Clod next time he comes at you with that line.
BTW, would use the exact same scenario for a heterosexual male also. If he is fused with the idea that he is NOT a Clod, but also fused with the idea that he is NOT a genius, then it might work just as well, have not had the chance to try. I would just say 'What is the likelihood you would use a line like that on someone? "Zero", right so what part of the bar room is a good analogy to your use of the term on yourself? "It wasn't a pickup line!" True enough, so what was it? and where did it come from? And what other stuff comes from that place? For gay clients, minor tweaks.
Am interested from those more experienced where this approach might have potential downsides or how it could be improved.
Cliff Jekel
P.S. Hat tip to Russ Harris who in ACT in Context podcast episode mentioned the idea of treating these thoughts as if they came from annoying teenagers. That's where I got the idea.
The Rip Current Metaphor (ACT is counter-intuitive)
The Rip Current Metaphor (ACT is counter-intuitive)This is a metaphor I devised, because so many of my clients are too young to know much about quick sand and don’t have their licenses yet so also don’t really understand skidding on the road. It works very well when you ask the client what they know about rip currents and then draw out the analogy from the information given by them. Young surfers love this metaphor and most clients can relate to how exhausted they are by their current control efforts.
When caught in a rip current, swimmers often intuitively swim towards the shore, unwittingly swimming directly against the rip. This is the main reason rips are so dangerous, because the strong current keeps pulling the swimmer back into the ocean, so even the strongest swimmer makes little progress, risking exhaustion and drowning. Experts advise us that a rip is ‘like a treadmill which the swimmer needs to step off’. This is done by swimming parallel to the shore until one is outside of the rip current, encouraged to aim for places where waves are breaking, which can assist one in being transported towards the shore. If the rip is too strong to allow the swimmer to swim away from it, advice is to relax and calmly float or tread water to conserve energy and wait till the rip loses its strength. Then swim leisurely in a diagonal direction away from the rip, but back to the shore.
Being caught up in a turmoil of emotions and thoughts can be very similar to a rip current. You might be able to clearly see the shore, i.e. the direction you want to take your life. Yet all your efforts just leave you exhausted, as you desperately try to fight your thoughts and feelings in order to reach your goals, almost like swimming into the rip current towards the shore. Our intuition and often the coping mechanisms we have learnt, urge us to try to get rid of thoughts and feelings as the only way to reach our goals. Yet, contrary to what you might believe, this is a very ineffective strategy. Some of the processes used in ACT therapy are counter-intuitive, asking you to go against what may feel like the right thing to do. At first some of these techniques might feel as if you are going deeper into the ocean rather than moving towards your goals. Sometimes it will be necessary to just calmly tread water and allow yourself to feel overwhelmed by your thoughts and feelings until the turmoil loses its strength. And at times you might have to make a slight course correction, swimming diagonally towards your goal rather than in a straight line. As you learn to notice what is happening in the here and now, you might be able to find the “places where waves are breaking”, the things that will aid you in getting to your goal more efficiently.
I'm sure you will have fun in drawing out more explicit analogies to Values, committed action and Self as context. I just thougth I would get the idea started.
Warm regards
Esthe Davis
The Sh*t Metaphor
The Sh*t MetaphorHere's a fun one. It's a little gross, perhaps. A client and I were talking about what minds do and I pulled the idea of using the comparison to organs. I think this is from Out of Your Mind.
Anyway, so the client says: "I get it, intestines make shit. Minds make thoughts."
We laugh and then start fooling around with the metaphor, like this: What happens if your intestines stop making shit? Not a good thing.
What happens when your intestines do make shit?
We agree that most people tend to check it out to see if things are working all right, and then they flush it.
Do your intestines make shit sometimes when you don't want them to?
Yes and sometimes won't make shit when I DO want them to.
Would it make sense to scoop your shit up, put it in your pocket, carry it around with you, and check on it all day?
Ewww, no!
So I'm thinking this is one of my more memorable Cfunc experiences.
That was a fun one. I've been laughing about it for a while.
Hope you all get a giggle too.
Joanne Steinwachs
The Store Metaphor
The Store MetaphorI kept hearing ACT therapists talk about "buying" thoughts, so I took this idea to its extreme and wrote out the following, which I sometimes bring into sessions with clients:
The Store Metaphor
By Shane Knox
Let's imagine that your mind is a giant store. Since this store is your mind, you're the only customer. Oh, and you also have virtually unlimited money! All the merchandise in the store symbolize your thoughts, emotions, memories, urges, etc.—everything that goes on in your mind. Some of the merchandise you like, some you don't. Some of it seems really important to you, and other items are trivial. Some products are useful, or fun, or trendy, or unhealthy. Just like a real store, you probably have positive or negative judgments about lots of the items in the store, and others you just feel neutral about.
As a customer of this store, you don't really have direct control over what merchandise the store has for sale. But what do you have control over? Well, you decide what to buy! Your purchases will probably influence the store's future inventory. For example, if you buy lots and lots of staplers, the store will likely order more. And if they continue to sell out of staplers, the store will probably make a bigger stapler section to accommodate the apparent demand. So as customer, you do have some control over what the store sells, but it's a slow power, and there are no guarantees—it's really ultimately up to the store what's on the shelves.
So you can't control what's on the shelves, but you do get to choose what to buy. You choose what to take home with you. You likely don't like certain products, so why do you buy them? Are there any thoughts or feelings that you've “bought” that have actually made your life less rich?
What might it mean to “buy” a thought or feeling? It means you've “taken it home with you”. To “buy” a thought or feeling is to think you own it, to strongly identify with it as part of who you are. It might also mean you feel you must act on it. Or to put it another way, you believe this thought or feeling as if it's real and not just a thought or feeling. It's to mistake it as a solid object rather than just a passing experience. (Spend some time thinking about what it means to “buy” a thought or feeling, using personal examples if you can.)
It's not easy to scale back our spending and make conscientious purchases—we're often tempted by products that deliver short-term benefits at the expense of long-term well-being. We sometimes think we need something we actually don't, or get addicted to buying things in general. Even if we try to avoid the store altogether, there are bound to be reminders about what to buy in the form of advertisements and societal messages.
Ultimately, though, the “merchandise” you buy is your decision.
Thanks for sharing this Metaphor! - Comment submitted by scottpalasik on February 19, 2013.
Dear Shane,
You have really developed a well thought out and descriptive metaphor here. I can picture the store rows of items (thoughts) on a shelves as far as the eye can see (kind of like a giant Sam's Club). I particularly enjoyed the practice of "Spending some time thinking about what it means to "buy" a thought or feeling". This gets at the crux of choices and how we can change our behaviors by examining our thoughts.
This "buy in" is so important in life. I know you said we have "unlimited money", what if we didn't. How might having a limited supply of currency change the metaphor if we can only spend a certain amount on the thoughts that service us best. What thoughts would we want to own? At the same time, what thoughts do we let sit on shelves collecting dust? We can't throw them away, however we don't have to buy them either.
Thanks again,
Scott
Scott Palasik PhD, CCC - SLP
University of Akron
School of Speech-Language Pathology and Audiology
A little Acceptance thrown in too..... Comment submitted by docberf on December 4, 2014.
I've used a very similar scenario with my ACT groups that I call "The Supermarket of the Mind". Very same shopping metaphor (I usually ask who has ever shopped for groceries at a supermarket...a pretty universal experience). I then proceed to ask:
1. When you shop for groceries, do you go through and put everything that's on the shelves into your cart each week? (Resounding "No" from everyone). Why not? Usually the responses come along the lines: "Because I can't use/don't need everything." "Just buy what I need that week", etc. We usually concur that the best strategy is to buy what we can use and leave the rest on the shelves.
2. I then take it a step further and ask, "And I bet before you leave the store you stop by the manager's office to complain about all the products that were on the shelves that you can't use and demand that he not carry them any more, since that would surely make your marketing much simpler to know that the store only carried what you needed, right?" Generally, no one agrees with that and as we explore why not, we hear "Because I might need some of that stuff on other weeks" or "Just because I can't use it right now, doesn't mean I won't need it sometime" or similar ideas (which is a very nice way of introducing context and present moment awareness into the metaphor too).
3. Finally, I ask: "And in this whole scenario, guess what your mind's job is?" This will usually be a bit of a go round as we consider different "jobs" in the supermarket (manager? shopper? etc.) and try to compare it to their experience of their mind. At some point (if it hasn't been suggested by one of the group), I'll offer: Doesn't your mind work kind of like the stockperson? He/she isn't concerned with what you need or what you can use, what's good for you or bad for you this week, or even what you like or don't like. Their only job is to KEEP THE SHELVES STOCKED WITH EVERYTHING AND ANYTHING (also helping with Acceptance and Willingness to encounter products week to week that we dont like, can't use, etc. but no big deal since no one forces us to buy them).
Helping to draw the distinction between stocking the shelves and shopping from the shelves helps with a number of core processes from defusion to self-as-context (shopper vs. stocker vs. contents of my cart).
It's one of my favorite metaphors to use because everyone can relate and really have fun exploring it.
Keith Berfield
The Titanic metaphor
The Titanic metaphorHere's a metaphor I've been using to describe the difference between ACT and other therapies.
What if you're on the Titanic?
Some approaches might suggest moving the deck chairs around. (laughs all around)
What would be a better approach?
Client usually comes up with the idea of steering better.
My offering to them is perhaps it would be a good idea to get off the boat completely.
My Best, Joanne
The mind as a GPS
The mind as a GPSSometimes I find it useful to see the voice in my head that constantly provides me with an analysis of the surroundings and tells me what I have to do to proceed safely (and to be right !) as one of those GPS systems you can have built into your car. A sampled voice will then give you constant advice about what to do at the next crossroads. These systems are very convenient and useful. But it's still important to keep one's eyes wide open. Some drivers ended in a river because a bridge had been suppressed and the system hadn't been updated. In the north of Europe, a truck driver got stuck in a narrow lane. For sure he was on the right way, but the road couldn't accommodate such a wide vehicle. And some accidents happen because a driver is too busy fiddling with the controls of the system and neglects to watch the road.
Of course that thought is perfectly logic and your mind tells you that it's not only a thought but the plain truth. But will doing what that thought tells you to do lead you in a direction dear to your heart ? Fiddling with the controls won't give you the answer...
Thought/Emotional Avoidance and Acceptance: Ball in a Pool
Thought/Emotional Avoidance and Acceptance: Ball in a PoolI often use this metaphor with clients to convey the counterproductivity of cognitive and emotional avoidance. It is similar to the Pink Elephants metaphor but also suggests the alternatives of acceptance and willingness.
Imagine what you're doing with these (thoughts/distressing memories/feelings) is like fighting with a ball in a pool. You don't like them, you don't want them and you want them out of your life. So you try and push this ball under water and out of your consciousness. However, the ball keeps floating back to the surface, so you have to keep pushing it down or holding it under the water. This struggling with the ball keeps it close to you and is tiring and futile. If you were to let go the ball, it would pop up, float on the surface near you and you probably wouldn't like it. But if you let it float there for a while, with your hands off, it would enventually drift away and out of your life. And even if it didn't, at least you'd be better able to enjoy your swim rather than spending your time fighting!
I hope you find this is helpful.
Thoughts and Feelings: Droplets
Thoughts and Feelings: DropletsThis metaphor can be used as a vehicle for meditation/mindfulness practice or in therapeutic conversation with a client.
Thoughts and feelings come into our awareness. They create ripples - other thoughts and feelings. We don't like "bad" thoughts and feelings, so we bat at them.
We interfere by splashing around. The droplet of (a"negative" thought or feeling) comes in and we can choose to observe it, or meddle with it. What is it like to stop splashing? To let the droplet come, the ripples happen, and let them naturally subside.
If you have feedback, I'd love to hear your thoughts about this metaphor: anna@moodtreatmentcenter.com. Clients tend to come up with some brilliant ways of making this their own!
Thoughts as sales representatives
Thoughts as sales representativesThis metaphor resulted from my work with the owner of a small business. I found it useful with other clients too.
Picture your thoughts as sales representatives. Some of them aren't really gifted for that job. You just tell them you are not interested or you are busy right now and they will apologize for having disturbed you and never bother you again.
But then there are the tough guys. If you refuse to give them an appointment in your office, they will pop up on the parking lot when you are going back to your car or even around your house wenn you are mowing the lawn and put their open briefcase under your nose with those fantastic products they want to sell you. Your life is becoming a hassle, you need to spend more and more time trying to escape them. Instead of doing productive work, you spend most of your time at the office door trying to get rid of them. Maybe it's easier to let them in, listen to what they want to tell you, thank them for coming and let them go... After all, you are the boss : It's up to you to decide which product you'll buy.
I sometimes add: And maybe one or the other of all these products they advertise could be a good business opportunity?
I've always liked this - Comment submitted by joshua.zurba on December 14, 2017.
I've always liked this metaphor. It makes sense, the mind is trying to hook you and suck you in the same way a salesperson can. To build a bit of self-compassion, I might also say the salesperson might have good intentions (e.g. the mind telling you you should drink to get rid of your anxiety is trying to release you from feeling pain) but that maybe they're not selling the most helpful products. In later sessions you can bring this metaphor back: "There's your salesperson mind trying to sell you a thought again. If you buy this thought, how much will it cost you?" Obviously cost in this sense isn't monetary, so I love the play on words.
YouTube Video - Comment submitted by LauraAnn on October 12, 2020.
Thoughts as Sales Representatives - an Acceptance & Commitment Therapy (ACT) Metaphor
https://www.youtube.com/watch?v=SyzwCZ1fAS0&feature=youtu.be&fbclid=IwAR3my7JO4eSEIio4uvfZ90vaP3muDNHo1vh7YbaixkGnQH7yTHwwUZbMpMc
Trumps
TrumpsTwo Mountains Metaphor
Two Mountains MetaphorQuoted from Twohig, M. (2004). ACT for OCD: Abbreviated Treatment Manual "It’s like you’re in the process of climbing up a big mountain that has lots of dangerous places on it. My job is to watch out for you and shout out directions if I can see places you might slip or hurt yourself. But I’m not able to do this because I’m standing at the top of your mountain, looking down at you. If I’m able to help you climb your mountain, it’s because I’m on my own mountain, just across a valley. I don’t have to know anything about exactly what it feels like to climb your mountain to see where you are about to step, and what might be a better path for you to take."
Waiting for the wrong train
Waiting for the wrong trainThis is a metaphor that grew out of working with various clients over the last couple of years and from my own reading. I was thinking of the idea in ACT that clients can get stuck in a place of "things must get better, then I'll get moving". In this sense our clients (and dare I say, often ourselves as well)get stuck on our 'buts'. Sort of like "I know where I want to go but....I have this thing....it must go away or get better before I can do X,Y,Z". So we wait for our problems to leave or change before we can go on our merry way. So much so that chances to actually move in our valued direction may be missed, life passes us by while we wait for things to improve or while we avoid our discomfort.
So before I go on anymore, here is the metaphor I came up with.
"Imagine you are going on a journey. Somewhere really special, where you really want to go, somewhere you've wanted to go your whole life. When you get to the train station you see two trains, one is a bit odd looking and strange, some of the seats look a bit hard and overall it looks a bit dirty and uncomfortable. On the next platform, there is a different train; it's a super train. It looks familiar, safe, reliable, the sort of train an accountant or an insurance sales man might prefer. The sign says it has air conditioning, a cinema, and a fancy all you can eat French restaurant that is free. You think, wow! I just have to take this train, I couldn’t possibly make my journey on that other one, no way! So you wait for this 'great' train to get ready to board and the odd looking train goes on its way. And you wait for the safe train some more and another odd train leaves the station, and another. All the while you are waiting for a chance to board this great reliable train so you can take your journey, as yet another odd looking one leaves. But here is the thing. What if the safe train can't ever board, what if it won't ever leave the station. What if you are waiting for the wrong train?"
Like most process in ACT there is no definitive right time to use this metaphor. It could be discussed like the man in the hole exercise, or I suppose it could be done more experientially, especially if your client has a clear idea of their values and can visualise stuff very clearly. However, I think what I am trying to get at is
1. You know where you want to go in life, what are you prepared to have/experience to get there?
2. If we can't ever have discomfort, where does that leave us?
3. How does waiting for the good ol' predicable train work in terms of actually moving towards our values and goals.
the metaphor was tweaked slightly after sharing it with the listserve for feedback. It was also realised by one person who gave me feedback, that the metaphor may lend it self to further tweaking. Essentially we have 2 trains, one that will help clients move forward that might be difficult and another one that they would rather wait for. It should be possible to alter the descriptions of the 2 opposing trains to better fit our clients difficulties.
So if the metaphor makes sense, if it seems to connect with some of the difficulties your clients are struggling with, then give it a go. If you do though, please feedback on how it went, what they made of it etc.
Trains leaving the here and now station metaphor
Trains leaving the here and now station metaphorTrains leaving the station metaphor--which one do you choose?Airan, Thanks for the train metaphors; I'm going to use them. The following similar metaphor popped up in my mind while reading your note: What about asking a client (or ourselves) to make a choice between two trains ready to leave the here and now station? One is an uncomfortable train and is moving in a valued direction; the other is your luxury, ultra-comfortable train and is moving exactly in the opposite direction. Which one are you going to choose? Best, Koke
TWO TRAINS - Comment submitted by DrEickleberry on February 20, 2019.
Koke:
This is a great addition to the train metaphor. In fact, I’ve found it to have terrific utility with substance abuse. The luxury train (the one that represents drug/alcohol use) is easy to get on and initially comfortable, however, because it is going in the wrong direction, it eventually leads to a place that is less comfortable and much further from where you want to be, which is in itself distressing. Staying on the luxury train indefinitelty also will eventually lead to distress....you’ll become bored, the train will break down, etc. The less savory train (represents the difficult path to sobriety) may not be as much fun initially, but leads to a place bettrer than the other train can ever take you. Hope this is useful!
Lori
Windmill Metaphor
Windmill MetaphorI work with children mostly between 8 and 13 years of age, many who have autism and struggle to navigate the social world - with dificulties like how to interpret and respond to others, how to frame theirs or others' communication - often they lack context from which to confidently respond and/or react to people.
I do a lot of teaching of flexibility vs. rigid thinking in social and peer situations. In my work I have shared the idea of the willow tree being strong becasue it is flexible and bends in the wind and storms, thus it's indestructable, yet the mighty oak, tall and rigid, can be brought down by a strong wind and a well-placed bolt of lightening, really not very strong ....
Lately I've added a new slant to this wisdom with a Windmill Metaphor.
Think of a windmill, tall, sleek, majestic, especially the modern ones. Not only does a windmill survive a fierce storm, but it most likely LOVES a good strong wind. In fact, the stronger the wind, the more power it generates - and this power is a completely "good power." It makes electricity that we all use, yet in a way that is gentle and does not hurt; it is soft, fluid, quiet (doesn't yell, scream, or cry) it doesn't damage the enviornment or pollute (doesn't punch, kick, or hit ) --- all the windmill needs is the most natural of all elements, the limitless wind (no resistance, only acceptance).
I use the windmill metaphor when working with kids who are being picked on or when they don't know how to respond to someone being mean or nasty. Of course, we all know violence isn't the answer, in fact in the ACT playbook, that which you resist only becomes stronger (think: inner monster/demon or our internal or external tug of war, right?)
In order to beat the monster, one must lay down the rope and stop pulling.
- I feel the windmill image goes a step further: Put down the rope, stop fighting/resisting, and be like a windmill.
The windmill metaphor asks: "How can you use that graceful and limitless energy to give yourself the might and power you need?" In fact, I have come up with an acronym for this:
"WWAWD"?
Kids like this imagery and they have no problem with the concept. It's simple, we all love windmills, they thrive off of the mightiest winds (bullies, mean people), yet just like a willow tree, they offer up no resistance. In fact, a windmill drawing session could also be easy to produce, drawing with the client a series of windmills while envisioning the quiet and confident power they hold for us.
- They just turn, and turn, and turn -
- Graceful, with no extra effort -
- Soft and yeilding, yet tall and strong -
Your life as a movie
Your life as a movieI've found this metaphor useful in values work and as a defusion exercise. Janet Wingrove's feedback (thank you Janet!) helped me to improve the wording.
Picture your life as a movie. The first episodes are already shot. (Here I usually summarize what I know of the – usually difficult – salient moments of the clients life). Now the movie is going on. Imagine you are the director and you can direct an actor that plays your part. But you're a special kind of director with a limited power. You can't go to the screenplay writer and ask him to change the life events happening to you or direct the other characters to act like you'd want them to do. The only actor you can have an influence on is the one playing your part. You can have him/her play exactly like the person you dream to be. Figure out how you would want him/her to act, in that precise situation you are experiencing now. How would you instruct the actor to act if you want the continuation of the movie to resemble what you would like your life to be, or to show the father / spouse / colleague / etc. you would like to be?
This metaphor has multiple sources.
(1) Doing values work with clients, I tried the tombstone exercise and the funeral exercise and had the feeling they didn't really ring a bell. It seemed to me that people understood them as one more appeal to pliance, to being a «good boy» or «good girl».
(2) I found an idea of Dan Millman interesting : «When I refer to practicing "everyday enlightenment," I'm speaking about actually consciously asking, "How would an enlightened being act in this moment?"—and then acting that way.»
(3) Alexandre Jollien is affected by a severe form of cerebral palsy due to birth damage and had to face the trauma of being separated from his parents at the age of 3 and raised in a faciltiy for disabled children. He finally made it to a degree in philosophy and published two books the title of which can be translated as «In praise of weakness» and «The trade of becoming a human being». He's now married and father of a young child. He explains in his crippled voice how the ancient greek philosophers have taught him that one could sculpt one's life in order to do a work of art out of it.
(4) This connected with Viktor Frankl's suggestion to think of ourselves as those who were being questioned by life - daily and hourly. And with the bus driver metaphor, each question of life being a new crossroad, a new opportunitiy to drive the bus in a valued direction. The reels of the past episodes come with us. I remember Frankl said that, in a novel or in a movie, it is sometimes what happens at the very end that gives a new meaning to the whole story.
The recalling of this metaphor in some difficult situations sometimes helped me to defuse of some tricky contents and to steer the course dear to me. I had the feeling it was less felt as pliance inducing by clients as the funeral and tombstone exercises. They sometimes answered to it with statements like «I would want him (her) to stay cool, to think positively etc.» which set the occasion for one more round of creative hopelessness work.
What I'm mainly afraid of is that the metaphor could be fueling self-accusations in all the cases where the passengers succeed in having the bus driven in the direction they want life to proceed.
I'm still interested in and grateful for any feedback
Videos - Metaphors
Videos - MetaphorsACT for the Public - Free Videos: Learning About and Applying ACT
- Chessboard
- Demons on the Boat (Joe Oliver)
- Passengers on the Bus (Oliver, Christodoulou, & Whitfield)
- Tug of war with a Monster (Louise Gardner - Your ACT Auntie Series)
- The Unwanted Party Guest (Joe Oliver)
- New animation of the Chessboard metaphor (Russ Harris)
More Videos
- Les Passagers du Bus | Choisissez l'aventure qui est la vôtre: https://www.youtube.com/watch?v=TYjIYp-46zc
LAMIC Resources
LAMIC ResourcesWelcome to the LAMIC Resources section of the ACBS website.
Your colleagues from Low-and-Middle-Income-Countries (LAMIC) have looked through all the resources on the ACBS site and chosen some really great quality resources for you to get some understanding of Acceptance and Commitment Therapy (ACT), Relational Frame Theory (RFT) and Focused Acceptance Commitment Therapy (FACT). It is our hope that these pages support your own committed action to learn and these will just be a start for you on your journey.
This webpage has resources in English. Volunteers from the Developing Nations Committee have translated resources in Portuguese and Spanish.
Scholarships and Grants for Low and Middle Income Countries
Scholarships and Grants for Low and Middle Income CountriesACBS Membership Scholarship
The scholarship recipients receive complimentary membership to ACBS for one full calendar year. Applicants must reside in "Low-Income Economies" or “Lower-Middle Income Economies” as defined by World Bank Country and Lending Groups. Read more about the eligibility requirements and the application.
Developing Nations World Conference Scholarship
Available scholarships include both pre-conference and conference fee waivers to the ACBS World Conference. Applicants must reside in "Low-Income Economies" or “Lower-Middle Income Economies” or “Upper-Middle Income Economies” as defined by World Bank Country and Lending Groups. Read more about the eligibility requirements and the application.
Diversity, Equity and Inclusion World Conference Scholarship
The available scholarships include conference fee waivers. To be eligible for these DEI World Conference Scholarships, applicants must complete an application detailing their motivations to attend the conference, as well as a plan for how to use the knowledge and resources gained at the conference in the pursuit of their careers. Read more about the eligibility requirements and the application.
Research Development Grants
ACBS provides three Research Development Grants, up to $5,000 USD each. One of these grants is reserved for qualifying projects for those researchers living/working in "Low-Income Economies" or “Lower-Middle Income Economies” or “Upper-Middle Income Economies” as defined by World Bank Country and Lending Groups. Read more about the eligibility requirements and application.
ACBS Foundation Grants
The ACBS Foundation provides grants, up to $2,000 USD each. The ACBS Foundation aims to promote CBS projects around the world. With the goal of facilitating interventions that promote well-being, we are proud to announce a funding mechanism for ground-breaking projects that share this aim in the realms of interventions, training, and research. These could include - but are not limited to - projects involving developing nations, refugees, or other disenfranchised or marginalized people; projects focusing on climate change; interventions in hitherto untested populations; novel applications or modalities of interventions; projects focused on dissemination; projects that address public policy; projects that measure outcomes of training; projects that examine interventions in naturally occurring groups (prosocial); projects that have the potential to improve diversity, equity, and inclusion and/or address institutional racism; projects that address biological correlates of CBS-relevant targets (multi-level approaches); or interventions using technology that would have a wide reach to help people in their natural contexts. Read more about the eligibility requirements and application.
For the full list of available ACBS Awards, Scholarships, and Grants, click here.
ACT for ALL Project
ACT for ALL ProjectACT for ALL is an ongoing effort to develop and share online resources for professionals from diverse nations to learn about ACT and to learn about adapting its application for various cultural contexts. With the support of the ACBS Developing Nations Committee and the Training Committee, ACT for ALL resources are developed through collaborations between volunteer peer reviewed ACT trainers (PRTs) and valued professionals from low and middle income countries (LAMIC).
There is more information about the development of this effort through the document attached below.
Values conversation with Fady Safwat and Jenna LeJeune (Recorded May 2023) 
Fady Safwat and Jenna LeJeune just completed a collaboration video about values for the ACT for All (Peer-Reviewed Trainer and LAMIC Practitioner) Project. This is a recorded conversation between Fady and Jenna about how they view values and work with values in their various contexts, in the U.S. and in Egypt. We hope listening to this conversation will give ACBS members some ideas about working with values in different cultural contexts.
Acceptance & Commitment Therapy Resources
Acceptance & Commitment Therapy ResourcesWelcome to the LAMIC Resource page for ACT. This page is aimed at practitioners from Low-and-Middle-Income-Countries (LAMIC) who are new to Acceptance and Commitment Therapy (ACT) and would like to learn more. It.jpg) is our hope that this page supports your own committed action to learn and makes the content more accessible for you.
is our hope that this page supports your own committed action to learn and makes the content more accessible for you.
ACT is pronounced as one word (not as an acronym) and has a very ACTive community. This means that new evidence, content, and resources are constantly being created. If you are looking for something that is not available on this page or have an idea of something that can be added please let us know.
We have tried our best to indicate whether each resource below applies to beginners or more intermediate practitioners. However, we recommend that you remain flexible and use the resources that are useful and meaningful for you and your context.
You will need to login as a member to see many of the linked resources, but some are available freely to the public (free resources are designated by 3 asterisks***). If you are interested in ACBS Membership you will find more information, including our values-based dues here. ACBS offers a number of membership scholarships - you can apply for a scholarship here.
Community
If you are seeking community to support your growth and learning, then please click this link https://contextualscience.org/chapters/sigs/affiliates
and explore the global ACT chapters and affiliates. If you would like to start with some self-directed learning, then please check out the resources below.
Books
Books for the beginner. These books are a useful ‘first look’ into ACT and how it can be applied. These are also readings that can be given to clients/patients/the general public who are seeking to know more and understand how to apply ACT to their lives.
- The Happiness Trap (Dr Russ Harris). Is a book that covers the basics and gives experiential exercises and is written for those with no training in mental health.***
- A Liberated Mind (Dr Steve Hayes), How to Pivot towards what matters. A self-directed learning book with a greater emphasis on explaining the more technical terms of ACT.***
Books for the beginner: technical stuff
The books below are useful for the practitioner who would like to start actively using ACT in their own professional space. They provide an insight into the theoretical foundations of the model and how it is applied in a real-world context:
- ACT Made Simple: An Easy-to-Read Primer on Acceptance and Commitment Therapy (Russ Harris). This book is aimed at newcomers but useful to experienced practitioners too. It offers a clear introduction to the 6 core processes and guidance on how to apply these with clients.***
- Learning ACT: An Acceptance and Commitment Therapy Skills Training Manual for Therapists (Jason B. Luoma, Robyn D. Walser, and Steven C. Hayes). This book has a skills-training focus. The authors recommend reading once you are familiar with some of the basic metaphors and processes of ACT.***
Once you have some ideas about specific things to try using ACT, feel free to use them yourself daily… this is by far the best way to really get the hang of the six processes and associated tools and techniques.
Articles
There are more that you might find interesting (and in other languages) so check out the full Publications list.
- Hayes, S. C. (2004). Behavior Therapy, 35, 639-665.
- Hayes, S. C. (2004). Acceptance and Commitment Therapy and the new behavior therapies: Mindfulness, acceptance and relationship. In S. C. Hayes, V. M. Follette, & M. Linehan (Eds.), Mindfulness and acceptance: Expanding the cognitive behavioral tradition (pp. 1-29). New York: Guilford.
- Hayes, S. C. (2000). Acceptance and Commitment Therapy in the treatment of experiential avoidance disorders.
- Hayes, S. C., Luoma, J., Bond, F., Masuda, A., & Lillis, J. (2006). Acceptance and Commitment Therapy: Model, processes, and outcomes. Behaviour Research and Therapy, 44(1), 1-25.
You will find a list of studies in low and middle income countries here.
Videos
There are many video presentations, examples & trainings available to the beginner practitioner. The list below aims to serve as a starting point, if your passion for ACT is ignited, we hope you continue to explore as more videos are created and shared throughout the ACBS community.
- Louise Gardner - Your ACT Auntie Series (ACT and Mindful Moments Videos)***
- Janina Scarlet, Yonatan Sobin - Superhero Therapy: Using Pop Culture to Strengthen Acceptance and Commitment Therapy
- Dr. Russ Harris - About ACT in simple terms***
- Tom Lavin - New Skills for Living - Experts on using ACT in daily life***
- Hank Robb - Being Where You Are and Doing What's Important***
- Louise Hayes - How we can use CBS to help humanity
- Robert Whelan - Thinking Big (Data) For Contextual Behavioral Science
- Rachel Collis - Why 21st Century Leaders Often Feel In Over Their Heads and How Psychological Flexibility Can Help
- Pam Katz - Creative Metaphors in ACT
- Luoma, Walser and Hayes - Learning ACT - Skills and Comptencies for Clinicians***
- Daniel J. Moran, Patricia Bach, Sonja V. Batten - Committed Action in Practice: Blending Evidence-Based Interventions into the ACT Model
-
Interview with Steve Hayes - ACT, RFT and their clinical applications (subtitles in Portuguese - Rolê Contextual Entrevista - Steven Hayes - ACT, RFT e suas aplicações clínicas)
If you are familiar with ACT already and are looking for some more intermediate videos to explore then try these:
- Stefan G. Hofmann - An Individual Complex Network Approach to Intervention Science
- Paul Atkins, Gareth Holman, Benjamin Schoendorff - Meaning and Resilience In Our Organizational and Community Work
- Dr. Peitao Zhu - Cultural Humility in Counseling and Clinical Supervision
- Maggie McCulloch, RSW - ACT for Psychosis: Supporting individuals and their families
- Jane Morton, MA - Wise Choices: ACT for people with symptoms of Borderline Personality Disorder
Online courses
You can search for online courses in the ACBS Community Events Calendar. There are many online courses out there…. Please reach out to the DNC (Developing Nations Committee) who may be able to provide some low cost / no cost options to you.
Podcasts
If you are looking for content you can listen to, there are a number of podcasts available. Browse the podcast links below to listen to insights from the leaders in our field.
John Dehlin & Jennifer Plumb - An introduction to ACT Part 1***
John Dehlin & Jennifer Plumb - An introduction to ACT Part 2***
Steven Hayes - The History and Development of ACT with Steven Hayes***
Sonja Batton - An Introduction to Acceptance with Sonja Batten***
Russ Harris - An Introduction to Defusion with Russ Harris***
Matthieu Villatte - An Introduction to Self-As-Context with Matthieu Villatte***
Kelly Wilson - An Introduction to Contacting the Present Moment with Kelly Wilson***
Joanne Dahl - An Introduction to Values with Joanne Dahl***
DJ Moran - An Introduction to Committed ACTion with Daniel J. Moran***
Robyn Walser - ACT for Coping with Trauma and PTSD with Robyn Walser***
Louise Hayes - ACT with Adolescents with Dr. Louise Hayes***
Worksheets & in-practice resources
For the practitioner who is already applying ACT or would like to start using it in a real-world setting. Below are some resources you can use to support these processes. Worksheets and handouts are a great way to facilitate Committed Action.
ACT Handouts***
Joseph Ciarrochi - Choice Point Model
Russ Harris - Handouts from Introductory and Advanced ACT Workshops
Protocols
Protocols are usually developed for research purposes and are useful in that context. They are not an essential part of ACT therapy; this is because ACT is designed to be flexibly applied and is not a rigid set of techniques. However, for the beginner practitioner protocols can be a useful starting point. They give an “inside-look” into the structure of a session and an unfolding of the process. Protocols can also be useful to explore how ACT can be tailored to a specific problem or client presentation. If you think protocols may be a useful resource for you and your work then please use the link below to explore.
Focused ACT Resources
Focused ACT ResourcesWelcome to the LAMIC Resource page for Focused Acceptance Commitment Therapy (FACT). FACT is a brief therapy that uses principles of ACT in a highly condensed version.

The strategies employed in FACT are delivered in fewer sessions when compared to traditional psychotherapies without compromising on the outcome. FACT is very useful in settings where time and resource-limitations are a limiting factor, it has been used in many different medical settings around the world.
This page is aimed at practitioners from Low-and-Middle-Income-Countries (LAMIC) who are new to FACT and would like to learn more and use it in their community. It is our hope that this page supports your own committed action to learn and makes the content more accessible for you.
You will need to login as a member to see many of the linked resources, but some are available freely to the public (free resources are designated by 3 asterisks***). If you are interested in ACBS Membership you will find more information, including our values-based dues here. ACBS offers a number of membership scholarships - you can apply for a scholarship here.
The following resources will aid you in learning more about FACT:
Books
Online courses
Several private providers run online courses and discounts are available for colleagues from LAMIC.
- Focused ACT for Brief Interventions by Kirk Strosahl and Patti Robinson. 6 weeks online course with evergreen access after enrolment. Some discount available for LAMIC, you would need to contact Patti Robinson for this.
- ACT as a brief intervention by Russ Harris. 6 weeks online course. Free courses are available for LAMIC participants, contact the chair of DNC for access.
Videos
There are only a couple of video presentations of FACT for the beginner practitioner. We are in the process of creating more, so please check this site regularly.
- ACT as a Brief Intervention: Clinical Training Workshop with Kirk Strosahl (Workshop Recording); 2011.
- FACT by Bruce Arroll (Video playlist); last uploaded 2017.***
- FACT by David Bauman (Video playlist); ongoing videos.***
Articles
As FACT is relatively new, the research base is still growing. Here are a couple of quality articles as a starting point.
- Monia Barreto, et al. (2019). A Single-Session of Acceptance and Commitment Therapy for Health-Related behavior change: An Open Trial with a nonconcurrent matched comparison group. Journal of Contextual Behavioral Science, https://doi.org/10.1016/j.jcbs.2019.06.003
- Heidi Maria Kyllönen, et al. (2018). A brief Acceptance and Commitment Therapy intervention for depression: a randomized controlled trial with 3-year follow-up for the intervention group. Journal of Contextual Behavioral Science, https://doi.org/10.1016/j.jcbs.2018.08.009
Relational Frame Theory Resources
Relational Frame Theory ResourcesWelcome to the LAMIC Resource page for RFT. This page is aimed at practitioners from Low-and-Middle-Income-Countries (LAMIC) who are new to Relational Frame Theory (RFT) and would like to learn more. It is our hope that this page supports your learning journey and makes the content more accessible for you. 
Relational Frame Theory (RFT) is a functional contextual approach to language and cognition. You can read about Functional contextualism here.
RFT is a theory of language and cognition which aims to integrate a wide range of psychological phenomena. It does use lots of jargon which makes it kind of scary to approach. But once you have a watch of the video recommended such as Tim’s and some of the introduction articles such as Jen’s, you might be surprised how quickly it makes sense and even explains some things about humans and their behaviours to you.
For example, relational frames refer to the human process of creating bidirectional links between phenomena. These relations form the building blocks of language, higher cognition and lots of helpful and problematic thoughts and behaviours.
The resources below aim to aid your learning, start with the videos, and save the books for later is probably most useful.
You will need to login as a member to see many of the linked resources, but some are available freely to the public (free resources are designated by 3 asterisks***). If you are interested in ACBS Membership you will find more information, including our values-based dues here. ACBS offers a number of membership scholarships - you can apply for a scholarship here.
Books
- Villatte, M., Villatte, J. L., & Hayes, S. C. (2019). Mastering the clinical conversation: Language as intervention. New York: The Guilford Press.***
- Dahl, J., Stewart, I., Martell, C., Kaplan, J. (2014). ACT and RFT in Relationships: Helping Clients Deepen Intimacy and Maintain Healthy Commitments Using Acceptance and Commitment Therapy and Relational Frame Theory.***
- Dymond, S., & Roche, B. (Eds.) (2013). Advances in relational frame theory: Research and application. New Harbinger Publications.***
- McHugh, L., & Stewart, I. (2012). The self and perspective taking: Contributions and applications from modern behavioral science. Oakland: New Harbinger Publications.***
- Törneke, N. (2010). Learning RFT: An Introduction to Relational Frame Theory and Its Clinical Application. Reno, NV: Context Press.***
- Rehfeldt, R. A., Barnes-Holmes, Y. (2009). Derived relational responding: Applications for learners with autism and other developmental disabilities. Oakland, CA: New Harbinger Publications, Inc.***
Videos
-
Tim McLauchlan - Learning RFT (Relational Frame Theory) – ACT is the car, RFT is the engine!
- What is Relational Frame Theory, this is a really excellent starting point and will give you the basics. -
Niklas Törneke, Robyn Walser - How to do an RFT- Enlighted Functional Analysis of Clinical Work
- How to do an RFT- Enlighted Functional Analysis of Clinical Work - Jennifer L. Villatte, Matthieu Villatte - Mastering the Clinical Conversation with RFT
- Ryan Sharma, Psy.D., ABPP - An Experiential Introduction to Relational Frame Theory
- Niklas Törneke - RFT and ACT – how do they go together?
- Paul Atkins, Ph.D., Dennis Tirch, Ph.D., Niklas Törneke, M.D., Paul Atkins, Ph.D., Louise McHugh, Ph.D. - The RFT of Meditation
- Behavior Analysis and Cognition - Videos in RFT***
- Frank W. Bond, Ph.D., Jonathan R. Dowling - ALIVE and Thriving: The Evolution of CBS in Theory and Practice
-
Interview with Matthieu Villatte - Clinical RFT in specific contexts (with Portuguese subtitles - Rolê Contextual Entrevista. Matthieu Villatte (Interview) - RFT Clínica em contextos específicos)
Articles
- Behavior Analysis and Cognition - Articles in RFT***
- Ian Stewart, National University of Ireland, Galway John McElwee, Private Consultant, Pennsylvania Siri Ming, Private Consultant, Maryland - Language Generativity, Response Generalization, and Derived Relational Responding***
- Jen Plumb - A Very Simple Overview of RFT (in non-technical language)***
- Articles Describing the Link Between RFT and ACT***
- Blackledge - An introduction to Relational Frame Theory: Basics and applications
World Health Organization: "Doing What Matters in Times of Stress" and Self-Help Plus (SH+)
World Health Organization: "Doing What Matters in Times of Stress" and Self-Help Plus (SH+)For more information about Self-Help Plus (SH+) and "Doing What Matters in Times of Stress" click here.
SELF-HELP PLUS (SH+) (2021)
A group-based stress management course for adults (World Health Organization)
https://www.who.int/publications/i/item/9789240035119
Overview
Self-Help Plus (SH+) is WHO’s 5-session stress management course for large groups of up to 30 people. It is delivered by supervised, non-specialist facilitators who complete a short training course and use pre-recorded audio and an illustrated guide (Doing What Matters in Times of Stress) to teach stress management skills. The course is suitable for adults who experiences stress, wherever they live and whatever their circumstances. It has been shown to reduce psychological distress and prevent the onset of mental disorders. The format of SH+ makes it well-suited for use alongside other mental health interventions, as a first step in a step.
Available in English, Arabic, Juba Arabic, French, Portuguese, Spanish, Turkish, Ukrainian.
Doing What Matters in Times of Stress (2020)
An Illustrated Guide
https://www.who.int/publications/i/item/9789240003927
https://iris.who.int/handle/10665/331901
Overview
Doing What Matters in Times of Stress: An Illustrated Guide is a stress management guide for coping with adversity. The guide aims to equip people with practical skills to help cope with stress. A few minutes each day are enough to practice the self-help techniques. The guide can be used alone or with the accompanying audio exercises.
Informed by evidence and extensive field testing, the guide is for anyone who experiences stress, wherever they live and whatever their circumstances.
Available in Arabic, Armenian, Chinese, Czech, Dari, English, Estonian, Farsi/Persian, Finnish, French, German, Georgian, Greek, Hungarian, Indonesian, Italian, Japanese, Juba Arabic, Korean, Lithuanian, Malay, Polish, Portuguese, Romanian, Russian, Slovak, Spanish, Swedish, Tigrinya, Tongan, Turkish, Ukrainian, Urdu, Vietnamese.
How to Use WHO Self-help Plus Protocol
Webinar presented by Russ Harris and Claudette Foley
April 13, 2022
https://contextualscience.org/video/how_to_use_who_selfhelp_plus_protocol_webinar
Overview
This is a webinar on WHO's ACT protocol for refugees. We will answer Frequently Asked Questions about the protocol–also known as “Self-help Plus”-and explore how to implement it.
Case Formulation Frameworks: Using the "Hexaflex"
Case Formulation Frameworks: Using the "Hexaflex"There are several ways to develop a case conceptualization of clients and their progress using the hexagon model.
ACT in Practice: Case Conceptualization in Acceptance and Commitment Therapy by Patty Bach and DJ Moran has a companion website that is hosted on the ACBS site, and provides a case conceptualization form freely available to you.
An external website also has an outline of a case formulation framework (based on the chapter in the Practical Guide to ACT) along with a form for therapists to use to complete the process (http://www.drluoma.com/actresources.html).
There are child pages below that provide several other ways of practicing developing a case conceptualization throughout therapy.
The Hexaflex Dimensional Approach to Diagnostics
The Hexaflex Dimensional Approach to Diagnosticsfrom
Wilson, K. G. (2006). The Heart of Acceptance and Commitment Therapy.
Wilson, K. G. (May, 2007) The hexaflex diagnostic: A fully dimensional approach to assessment, treatment, and case conceptualization. Presidential address presented at the annual convention of the Association for Contextual Behavioral Science, Houston, TX.
Empirical clinical psychology has largely been focused on measurement of the frequency and severity of various signs and symptoms and the treatment of psychological syndromes defined by clusters of signs and symptoms (DSM disorders for the most part). These syndromes have increasingly organized clinical psychology in spite of much criticism. It is imperative for us to understand that this is not as trivial as would be yet another theory of psychopathology. In such an instance, the presence of the theory might organize the activities of a relatively small group of individuals who share the area of research interest. Supposedly atheoretical syndromal classification, as seen in the DSM, has had a much more far reaching impact. Our central federal funding agency, the National Institutes of Mental Health, is organized around these categories, as are our abnormal psychology textbooks, journals, assessment instruments, and reimbursement for professional services. Such hegemony is wholly unwarranted based upon available evidence. Concerns about syndromal classification of psychological problems has been around for a good long time. However, only recently has dawn begun to break within the DSM effort.
The failure of syndromal classification carries with it a call for alternatives. At the University of Mississippi Center for Contextual Psychology and Acceptance and Commitment Therapy Treatment Development Group, we are exploring an alternative approach. Based on the idea that multiple systems of classification ought to compete with the gold standard being the treatment utility of the system of problem classification, we are currently pursuing the development and testing of the hexaflex model as the kernel of a fully dimensional diagnostic system within which there exists close linkage between diagnosis, assessment, and intervention.
Posted below are 1) slides from the plenary session in which the Hexaflex Diagnostic was presented at the ACT Summer Institute and 2) draft versions of clinician worksheets designed to facilitate use of the hexaflex model in this way. Please feel free to offer any feedback you might have as to the utility of the model and tools presented here. Send feedback to Kelly Wilson at kwilson@olemiss.edu These documents are extracted from a book in progress "The Heart of ACT," please copy and use at will for clinical practice and research. Distribute only with express consent of the author.
peace all,
Kelly
ACT ADVISOR Psychological Flexibility Measure
ACT ADVISOR Psychological Flexibility MeasureACT ADVISOR
ACT ADVISOR is a hexaflex-based self-report measure of psychological flexibility, its name being an acronym for the hexaflex processes (Acceptance; Commitment & Taking action; Attention to present; Defusion; Values Identification; Self as Observer; and Resulting psychological flexibility). It may be used both in case formulation and in tracking progress during therapy.
On being presented with this “double hexaflex” diagram, users are asked to choose where they would place themselves on the six different scales representing these core ACT processes, each with “opposite” statements at either end. Scoring is simply a matter of recording the user’s numerical responses and totalling them to give their Resulting psychological flexibility score. If ACT ADVISOR is administered repeatedly, scores can be tracked using the charts provided.
The idea for using the hexaflex as a diagnostic/ case formulation tool was, I believe, originally Kelly Wilson's and his materials (see The Hexaflex Dimensional Approach to Diagnostics) influenced the development of this instrument. Steve Hayes made helpful suggestions about the anchor statements for each process in earlier drafts, and I am also grateful for the ACT listserv community’s interest and input.
ACT ADVISOR statement rating form offers an alternative format. In this version users are asked to rate 12 statements independently of each other and without the possible steer of the double hexaflex diagram. Instructions for scoring this version are provided separately, with the Resulting psychological flexibility score here being converted to a percentage.
ACBS members login their account and then click here to download the ACT ADVISOR and related documents.
Submitted by David Chantry
ACT Case Conceptualization Grid
ACT Case Conceptualization GridAttached is a simple, user-friendly 9-box case conceptualization grid from a functional contextual perspective. The top row emphasizes the situational/historical context of the presenting problem(s); the middle row allows for a basic functional analysis of unworkable behaviors (taking into account the contextual variables identified in the top row); and the bottom row emphasizes values/process-directed treatment planning.
ACT Case Formulation Framework
ACT Case Formulation FrameworkI. Context for case formulation
The goal of ACT is to help clients consistently choose to act effectively (concrete behaviors in alignment with their values) in the presence of difficult or interfering private events.
II. Assessment and Treatment Decision Tree
Beginning with the target problem, as specified by the client or significant others, refine these complaints and concerns into functional response classes that are sensitive to an ACT formulation and to the client's contextual circumstances, and link treatment components to that analysis
A. Consider general behavioral themes and patterns, client history, current life context, and in session behavior that might bear on the functional interpretation of specific targets in ACT terms. These may include:
1. General level of experiential avoidance (core unacceptable emotions, thoughts, memories, etc.; what are the consequences of having such experiences that the client is unwilling to risk)
2. Level of overt behavioral avoidance displayed (what parts of life has the client dropped out of)
3. Level of internally based emotional control strategies (i.e., negative distraction, negative self instruction, excessive self monitoring, dissociation, etc)
4. Level of external emotional control strategies (drinking, drug taking, smoking, self-mutilation, etc.)
5. Loss of life direction (general lack of values; areas of life the patient "checked out" of such as marriage, family, self care, spiritual)
6. Fusion with evaluating thoughts and conceptual categories (domination of "right and wrong" even when that is harmful; high levels of reason-giving; unusual importance of "understanding," etc.)B. Consider the possible functions of these targets and their treatment implications.
1. Is this target linked to specific application of the tendencies listed under "A" above
2. If so, what are the specific content domains and dimensions of avoided private events, feared consequences of experiencing avoided private events, fused thoughts, reasons and explanations, and feared consequences of defusing from literally held thoughts or rules
3. If so, in what other behavioral domains are these same functions seen?
4. Are there other, more direct, functions that are also involved (e.g., social support, financial consequences)
5. Given the functions that are identified, what are the relative potential contributions of:a. generating creative hopelessness (client still resistant to unworkable nature of change agenda)
b. understanding that excessive attempts at control are the problem (client does not understand experientially the paradoxical effects of control)
c. experiential contact with the non-toxic nature of private events through acceptance and exposure (client is unable to separate self from reactions, memories, unpleasant thoughts)
d. developing willingness (client is afraid to change behavior because of beliefs about the consequences of facing feared events)
e. engaging in committed action based in values (client has no substantial life plan and needs help to rediscover a value based way of living)C. Consider the factors that may be perpetuating the use of unworkable change strategies and their treatment implications
1. Client's history of rule following and being right
(if this is an issue, consider confronting reason giving through defusion strategies; pit being right versus cost to vitality; consider need for self-as-context and mindfulness work to reduce attachment to a conceptualized self)
2. Level of conviction in the ultimate workability of such strategies
(if this is an issue, consider the need to undermine the improperly targeted change agenda, i.e., creative hopelessness)
3. Belief that change is not possible
(if this is an issue, consider defusion strategies; revisit cost of not trying; arrange behavioral experiments)
4. Fear of the consequence of change
(if this is an issue, consider acceptance, exposure, defusion)
5. Short term effect of ultimately unworkable change strategies is positive
(if this is an issue, consider values work)D. Consider general client strengths and weaknesses, and current client context
1. Social, financial, and vocational resources available to mobilize in treatment
2. Life skills (if this is an issue, consider those that may need to be addressed through first order change efforts such as relaxation, social skills, time management, personal problem solving)E. Consider motivation to change and factors that might negatively impact it
1. The "cost" of target behaviors in terms of daily functioning (if this is low or not properly contacted, consider paradox, exposure, evocative exercises before work that assume significant personal motivation)
2. Experience in the unworkability of improperly focused change efforts (if this is low, move directly to diary assessment of the workability of struggle, to experiments designed to test that, or if this does not work, to referral)
3. Clarity and importance of valued ends that are not being achieved due to functional target behavior, and their place in the client's larger set of values (if this is low, as it often is, consider values clarification. If it is necessary to the process of treatment itself, consider putting values clarification earlier in the treatment).
4. Strength and importance of therapeutic relationship (if not positive, attempt to develop, e.g., through use of self disclosure; if positive, consider integrating ACT change steps with direct support and feedback in session)F. Consider positive behavior change factors
1. Level of insight and recognition (if insight is facilitative, move through or over early stages to more experiential stages; if it is not facilitative, consider confronting reason giving through defusion strategies; pit being right versus cost to vitality; consider need for self-as-context and mindfulness work to reduce attachment to a conceptualized self)
2. Past experience in solving similar problems (if they are positive and safe from an ACT perspective, consider moving directly to change efforts that are overtly modeled after previous successes)
3. Previous exposure to mindfulness/spirituality concepts (if they are positive and safe from an ACT perspective, consider linking these experiences to change efforts; if they are weak or unsafe - such as confusing spirituality with dogma - consider building self-as-context and mindfulness skills)
III. Building interventions into life change and transformation strategy
(Originally posted by Steve Hayes and moved to this location by J. Luoma)A. Set specific goals in accord with general values
B. Take actions and contact barriers
C. Dissolve barriers through acceptance and defusion
D. Repeat and generalize in various domains
The actView (the board for The ACT Game)
The actView (the board for The ACT Game)Assessment and Monitoring Tools
Assessment and Monitoring ToolsIf you want formal assessment measures, this is the wrong page. These are more like helpful clinical tools. You can find formal assessment devices under the assessment resources section, click here
ACT Daily Diary & Weekly Report
ACT Daily Diary & Weekly ReportThe ACT daily diary and weekly report (see attachments below) can be clinically useful in monitoring progress.
ACT Vowels Assessment (AVA)
ACT Vowels Assessment (AVA)This brief questionnaire was designed to quickly assess skills related to psychological flexibility: awareness (of here-and-now experience), openness (to private events), engagement (in valued actions), and perspective-taking (of self/other). It can be freely used as a clinical assessment tool and for treatment planning purposes.
All feedback is welcomed!
Behavioral Health Progress Note Template
Behavioral Health Progress Note TemplatePlease log in as a ACBS member, and click the attachment link below in order to download the Behavioral Health Progress Note Template.
Clinical significance tester
Clinical significance testerThis tool will allow you to see if you have made a significant difference in your clients life. It looks at two outcome scores (e.g. pre vrs post). It will tell you:
1) If there was significant change from Time 1 to Time 2
2) if the symptoms have reduced to a point that you would consider the client symptoms to be no worse than what you would find in a normal population
The tool allows you to look at a wide variety of outcome measures, such as the beck depression inventory, trait anxiety scale of the STAI, and many others You can also print out a report for your client file. Simply complete name and date and then print the first page of the spreadsheet.
I hope you find this useful best Joseph
Flexibility and Alliance Session Tool (FAST)
Flexibility and Alliance Session Tool (FAST)This brief clinical instrument was designed for use in follow-up sessions to assess skills related to the three pillars of psychological flexibility (openness, awareness, engagement), as well as key features of the therapeutic alliance (consistent with ACT and evidence-based), while evoking consideration of a goal for the current session, and a space for progress notes. Please use freely, and feedback is always welcomed.
Getting to Know Your Mind
Getting to Know Your MindThe following worksheet, titled "Getting to Know Your Mind," is an attempt to create an ACT-consistent "thought record" that can assist the client in practicing defusion after they leave the therapy session. ACT clinicians typically engage their clients in defusion work by encouraging them to relate to their thoughts in a variety of ways while emphasizing the automatic nature of thoughts, the harmful effects of avoiding or struggling with thoughts, the subtle experiential differences between fusion and defusion, and using workability/usefulness to measure whether or not a thought should be "used" or bought into. This is a lot for clients to remember and by its very nature can be difficult to grasp after just an hour-long therapy session. The hope is that this form can function as a boiled down, concrete version of defusion work seen in the therapy room and assist the client in making defusion a well-practiced part of their repertoire.
Modification of Lundgren Bulls Eye exercise
Modification of Lundgren Bulls Eye exerciseI made some adaptations to the Bull's Eye exercise for my own clinical use - this seemed to suit my purposes well.
Traducción al Español de Kasket's Bullseye
Traducción al Español de Kasket's Bullseye marcelogalloSelf-Care Monitoring Forms
Self-Care Monitoring FormsAttached, please find a copy of self-monitoring forms I use with a wide range of patients. I direct patients to monitor those self-care behaviors relevant to their treatment (hygiene, eating, going to sleep at reasonable hour, exercise, meditation/centering, alcohol use). There is ample room for adding other behaviors or to permit some journaling/notes. *I recently replaced the GIF formatted forms with forms converted to PDF format (using free PDF writer at www.gohtm.com).
Treatment Protocol and Manuals
Treatment Protocol and ManualsACT is an orientation to psychotherapy that is based on functional contextualism as a philosophy and RFT as a theory. As such, it is not a specific set of techniques. ACT protocols target the processes of language that are hypothesized to be involved in psychopathology and its amelioration, as described in the psychological flexibility model. ACT protocols are thus instances of a general intervention strategy which is designed to be flexibly applied. ACT protocols can vary from short interventions done in minutes or hours, to those that take many sessions. ACT can be used in groups, individual sessions, classroom settings, couples therapy, bibliotherapy, workplace trainings, and much more.
When an ACT strategy is applied to a given problem it can include specific interventions tailored to fit the needs and resources of the context and population -- resulting in varied protocols across populations. Furthermore, there will be variation even within protocols for specific populations based on the creativity of the researcher/clinician and relative emphasis on various ACT/RFT-sensible processes. For all of these reasons and many more, the world ACT community has chosen not to ossify the treatment through processes of centralization, certification and the like, preferring to trust its development to open an scientific processes. These include sharing of protocols, identification of processes of change, outcome research, basic research, and so on.
Protocols cited or displayed here are not the ACT approach to any given problem, but an ACT approach in the eyes of the serious researchers who post them. They are not "official" or "recognized" or approved by anyone by virtue of their posting here, but are offered as a resource to the world ACT community so that development of the approach can be accelerated. Clinical use of the protocols is the responsibility of those who choose to use them. If you plan to use these protocols in research, you should of course interact with the listed authors.
Since the ACBS community values intervention development as an empirical process, be sure to check out the latest evidence for the ACT model here.
ACBS Members: If you have an ACT treatment protocol you would like listed here, log in, and click on the "add child page" link at the bottom of this page. When adding your content, remember that you can attach relevant files and documents.
Introducing ACT to clients
Introducing ACT to clientsA brief introduction to ACT from the March 5, 2007 issue of the Sunday Telegraph in the UK
A brief introduction to ACT from the March 5, 2007 issue of the Sunday Telegraph in the UKSee attachment below
See also Spanish version submitted by Ramiro
A short introduction to ACT to be handed out after a first session
A short introduction to ACT to be handed out after a first sessionRuss Harris has this to say about the form which is attached below: I've attached a word doc of a brief summary of ACT that I give my clients on the first session. Anyone can easily re-edit it to suit their clientele. (I also usually give them a copy of the "Embracing your Demons" article; it's pitched at a level the average layperson can understand.)
Introducing Acceptance and Commitment Therapy Spanish Version
Introducing Acceptance and Commitment Therapy Spanish Version marcelogalloACT in plain language
ACT in plain languageACT in plain language Submitted by Joel Guarna on February 1, 2006 - 10:38pm. I agree that explaining ACT plainly is difficult. With my clients, I often compare and contrast ACT with CBT more generally, since CBT is more widely known. I discuss similarities and refer to some common roots to both. I then illustrate some contrasts to traditional CBT by saying that an ACT approach is "not so much about changing the content of thinking (give examples, +/- thinking, etc) or fixing 'distortions' as about changing your relationship to your thoughts, feelings, memories, and other so-called private events (relate these to their presenting issues). ACT is less about making anxiety or depression go away and more about getting you untangled from the thoughts, feelings and rxns you have and getting you (client) moving in a direction that is important to you." I give a very lay summary that ACT is related to a basic science and theory about human language and thinking (I do NOT attempt to explain RFT in much detail) and their role in our suffering (I sometimes give examples of our pain/suffering and how it differs from nonverbal animals...if the client seems interested and appears to be following). I add that, since human language seems to complicate our dealing with private events, doing ACT as a "talk therapy" is tricky: "so, if you are up for it, we will use a lot of exercises, mindfulness practice, metaphors, and other methods to keep us both from getting tangled up in the words and ideas." I try to relate all of this to their personal issues as much as possible and use examples. I discuss this in "we" terms throughout. Once their interest is piqued (& it usually is) and I am satisfied they have a sufficient grasp on the approach to give informed consent, I implore them to hold whatever "understanding" of this that they now have VERY lightly. I then try to back out of all this wordiness and shift back into a more experiential mode. The process is a difficult balancing act b/n providing enough info for informed consent and getting ahead of ourselves and getting too didactic and wordy.
Explaining ACT - A comment submitted by Nicole Rensenbrink on October 2, 2010 - 10:37am.
I have a fairly low educated clientele and teens. I'm describing treatment to them in these terms:
I use a kind of therapy (ACT) that helps people figure out what's really important to them, develop goals that'll have them live according to what's most important, and then work through the barriers that get in their way of achieving these goals. There are three typical barriers:
1) Feelings: Lots of times people can't let their feelings be what they are so they act them out or create other problems for themselves by avoiding them.
2) Thoughts: Our brains are constantly busy and people often get so wedded to what their brains are telling them that they loose sight of what's really important to them.
3) Being present: Sometimes people are so distracted or preoccupied that they aren't there enough to follow through with what's important.
So that's I'll be doing with you in counseling, if you're interested.
ACT listings as an Evidence Based Treatment
ACT listings as an Evidence Based TreatmentThis list was updated in November 2021. The State of ACT Evidence webpage has an up-to-date list.
A number of different organizations, external to ACBS, have stated that ACT is empirically supported in certain areas or as a whole according to their standards. These include:
i. American Psychological Association, Society of Clinical Psychology (Div. 12), Research Supported Psychological Treatments:
Chronic Pain - Strong Research Support
Depression - Modest Research Support
Mixed anxiety - Modest Research Support
Obsessive-Compulsive Disorder - Modest Research Support
Psychosis - Modest Research Support
For more information on what the "modest" and "strong" labels mean, click here
ii. California Evidence-Based Clearinghouse for Child Welfare (click here for the report)
Depression Treatment (Adult) - Scientific Rating 1 (Well Supported by Research Evidence)
iii. U.S. VA/DoD Clinical Practice Guideline for the Management of Major Depressive Disorder
http://www.healthquality.va.gov/guidelines/MH/mdd/MDDCPGClinicianSummaryFINAL5192016.pdf
iv. Title IV-E U.S. Department of Health and Human Services (HHS) Prevention Services Clearinghouse (under review, 2021: mental health; substance use).
v. The World Health Organization
Pain (Children and Adolescents) - WHO lists ACT as empirically supported ("moderate certainty") in the reduction of functional disability in children and adolescents with chronic pain (click here for the 2020 report).
vi. The UK National Institute for Health and Care Excellence (NICE)
Pain - NICE recommends ACT for people aged 16 years and over with chronic primary pain. (click here for the full report).
Tinnitus - NICE recommends group-based ACT for tinnitus-related distress. (click here for the full report).
vii. Australian Psychological Society, Evidence Based Psychological Interventions in the Treatment of Mental Disorders (2018):
Adults
Anxiety disorders - Generalised anxiety disorder – Level II Evidence
Anxiety disorders - Social anxiety disorder – Level II Evidence
Anxiety disorders - Panic disorder – Level II Evidence
Borderline personality disorder – Level II Evidence
Depression – Level II Evidence
Hypochondriasis – Level II Evidence
Obsessive compulsive disorder – Level II Evidence
Pain Disorders – Level II Evidence
Psychotic disorders – Level II Evidence
Substance use disorders – Level II Evidence
Binge eating disorder – Level IV Evidence
Body dysmorphic disorder – Level IV Evidence
Children (age 10-14 years)
Pain Disorders – Level II Evidence
viii. Netherlands Institute of Psychologists: Sections of Neuropsychology and Rehabilitation, Richtlijn Neuropsychologie Revalidate (2017)
The Netherlands Institute of Psychologists (NIP) recommends ACT for patients with MS with depressive symptoms
ix. Sweden Association of Physiotherapists, Fysioterapi Profession och vetenskap (2016)
The Swedish Association of Physiotherapy (physical therapy) includes ACT as a physiotherapeutic theory and practice in the definition of the profession.
x. SAMHSA's National Registry of Evidence-based Programs and Practices, ACT, last review July 2010. (NREPP was shut down in 2018, so this will not be updated unfortunately)
ACT orientation diagrams
ACT orientation diagramsIn case they are of use to anyone, I am attaching a couple of ACT orientation diagrams - variations on a theme really.
I hasten to say that these are not in any way intended to challenge the Hexaflex. Rather, they are intended for use with clients (or colleagues etc) to give a quick introduction or summary of what ACT is all about. Perhaps they might also have a role in therapy (individual or group), say in aiding discrimination training (e.g., "whereabouts on the diagram are you now?").
Get Out of Your Mind and Into Your Life (4x4) diagram:
Steve was kind enough to look at an earlier draft of this diagram which, as the name suggests, is intended to provide an overview of the book. Perhaps it could also be used as a structure for collecting client examples (e.g., pain, unworkable control attempts, etc). (I nicknamed it 4x4 because of the 4 circles and 4 arrows and it's quicker to write in the notes!) The 4 arrows of course represent 4 of the hexaflex processes, being the ACT skills enabling the client to get out of their mind (lower circles - pain/ struggle > suffering) and into their life (upper circles - values/ commitment > action).
(Putting this together made me wonder if the sequence of the arrows could suggest a sequence for the teaching of ACT skills, each building on the previous one - i.e., being in the present moment facilitating the observer perspective - in turn facilitating defusion - in turn facilitating acceptance.)
Four Cycles diagram:
Similar idea but generally a bit more detailed, though amalgamating the "self-as-context" and "being present" processes in a single "noticing" item (and a similar amalgamation - "Overthinking" - in the Struggle cycle). In this one the pivot point is in the middle ("Pain") and from there you either shuttle round the Struggle and Suffering cycles - the former specifically includes the processes associated with psychopathology according to ACT (e.g., fusion) - or, after some ACT (it is hoped), the Acceptance and Commitment cycles.
-------------------------------------------------------------------------------------
I got a bit of feedback regarding these diagrams from my ACT follow-up group today. The view seemed to be that the 4x4 diagram provides a quicker reminder of the central ACT messages, that might be more useful in times of trouble, whereas the Four Cycles looks more complicated, but might have a role when learning ACT in more relaxed contexts. On the issue of using "noticing" to represent "self-as-context" and "being present", my group felt that "noticing" has the helpful connotation of something that is readily accessible in everyday life, whereas accessing an observer self seemed to suggest something more formal and effortful - perhaps less natural in everyday life. However, it was also said that being introduced to living in the present and the observer-self separately might be better when first learning ACT, moving to the more accessible noticing concept later.
Finally, I must mention that conversations with Mark Webster have influenced the development of these diagrams, and I believe that he in turn has been influenced by the Life Manual approach of Kevin Polk and colleagues.
Comparing ACT and CBT
Comparing ACT and CBTFrom my website - https://www.joelguarna.com/:
Treatment Approaches
Cognitive-Behavioral Therapy
What is Cognitive-Behavioral Therapy (CBT)? The history of CBT dates back to the seminal work of B.F. Skinner, the father of modern behavior therapy. At that time, behavior therapy was a reaction to the traditional Freudian forms of psychotherapy that were only loosely based on scientific principles and were difficult to subject to rigorous scientific study. Skinner held psychology accountable as a science of human behavior, forever changing the face of psychotherapy. Techniques drawn from Skinner's basic behavioral science continue to be employed with good effect in modern psychotherapy. Skinner's account, however, had its limitations. The most notable limitation was that his account of human language and cognition failed to generate a vigorous line of basic research, limiting its evolution to forms that could be employed with patients with complicated psychological problems. Instead, the field opened to the work of Albert Ellis and Aaron T. Beck, the founders of modern cognitive therapy. Ellis and Beck, and their many successors, transformed the practice of psychotherapy by emphasizing therapy techniques that aimed to change the content and manner of one's thinking, not just their overt behavior. Cognitive therapy and behavior therapy continued to cross-fertilize each other over the past several decades. Modern CBT incorporates both cognitive and behavioral techniques. CBT has become the most well-known, mainstream approach to therapy, partly because it has, by far, the strongest research support for its effectiveness in treating a wide range of emotional and behavioral problems. CBT has been found effective in treating depression, anxiety disorders, the effects of trauma, substance abuse and addiction, complications related to medical conditions, and many other conditions.
Acceptance and Commitment Therapy
What is Acceptance and Commitment Therapy (ACT, said as the word "act")? ACT, just approaching its 30th anniversary since its inception, is an innovative form of behavioral and cognitive therapy that has built upon both the strengths and the weaknesses of traditional cognitive-behavioral therapy (CBT). ACT is based on a behavioral account of human language and cognition called Relational Frame Theory (RFT), which has "filled in the holes" left by Skinner's theories. RFT, in contrast to Skinner's accounts, has generated a vigorous body of basic research into human language and cognition, providing fuel for the development of new treatment approaches. The "fruit" of this progress can be found in the philosophy and basic concepts underlying ACT. ACT has moved away from the traditional CBT emphasis on changing or correcting one's thoughts in order to alleviate suffering. Instead, ACT aims to alter the functions of our private experiences (thoughts, feelings, memories, bodily reactions), so they no longer entangle us. Said another way, ACT aims to change our relationship with these private events so we can become free from their grip, and free from the patterns that bind us and prevent us from living a flexible, meaningful, and enjoyable life. In the service of these aims, ACT incorporates acceptance strategies, mindfulness techniques, and a wide range of behavioral approaches already known to be effective from CBT. ACT is one of a family of interventions inside the CBT tradition writ large that are focusing on the person's relationship to experiences rather than on the content of these experiences. The data on ACT and related approaches are moving CBT itself toward a new model that emphasizes being open, centered, mindful and actively pursuing values. Because of that, ACT and CBT as a larger tradition are becoming more difficult to distinguish over time.
Communication au symposium Pleine Conscience des 37èmes Journées Scientifiques de l'AFTCC, Paris 12 décembre 2009
Communication au symposium Pleine Conscience des 37èmes Journées Scientifiques de l'AFTCC, Paris 12 décembre 2009
Étude d'analogues expérimentaux de la restructuration cognitive et de l'acceptation sur l'émotion et la croyance dans une pensée évoquées par un souvenir douloureux
L. CORNU (1), B. PUTOIS (1), B. SCHOENDORFF (2)
(1) Université Louis Lumière, Lyon
(2) Université Claude Bernard, Lyon
Communicant : Lydie CORNU Lydie Cornu
Problématique :
Les TCC de la 3ème vague promeuvent l’acceptation plutôt que la remise en cause des pensées et émotions douloureuses. Cette étude visait à mesurer l’impact relatif d’analogues expérimentaux de l’acceptation et de la restructuration cognitive.
Méthode :
Sujets : 44 (32 après critères d’exclusion) étudiants sains de l'Université Louis Lumière Lyon.
Matériel: Une fiche dérivée de la fiche de Beck à cinq colonnes était donnée à compléter pour un groupe et une fiche similaire mais avec des instructions d'acceptation (accueillir sensations, pensées et émotions) à un deuxième groupe. Les instructions étaient également présentées au moyen d'enregistrements audio.
Procédure : Les participants, assignés de manière aléatoire à l'un de deux groupes, Restructuration ou Acceptation, étaient invités à évoquer un souvenir difficile et à l'écrire sur la fiche, avec la pensée qui leur était venue, puis à coter sur 10 leur niveau d'émotion et de croyance dans la pensée. Le commentaire les guidait à travers les étapes de
chaque condition, puis les invitait de nouveau à coter émotion et croyance, ainsi que 15 jours plus tard.
Résultats :
Une ANOVA à mesures répétées a montré un effet principal du temps sur l'émotion évoquée F(2,60)=9.85, p<.0001, sans effet de tâche. Il y avait une interaction marginale Tâche X Temps F(2,60)=3.07, p=0.0537, indiquant que l'émotion baissait plus pour le groupe acceptation relativement au groupe restructuration. Les analyses de contraste révélèrent que la seule interaction significative était entre la phase pré-test et suivi. F(1,30)=7.56, p<0.01.
Un effet principal du temps sur la croyance F(2,60)=5.9810, p<.001, sans effet principal de la tâche ni interaction Tâche x Temps indiquait qu'il n'y avait pas de différence entre les deux groupes de réduction de la croyance.
Discussion :
Cette première exploration suggère que restructuration cognitive et acceptation réduisent tant l'émotion évoquée que la croyance dans la pensée négative évoquée par un souvenir difficile. Au suivi, cette expérience suggère que l'acceptation a un impact supérieur à la restructuration sur la seule réduction du niveau de l'émotion, mais pas sur la croyance dans la pensée.
Metaphors for Introducing ACT to Clients
Metaphors for Introducing ACT to ClientsSome metaphors that can be used when introducing ACT to clients include:
These and many others are available in the Metaphors section of Resources for Clinicians.
Purpose, Privilege, Presence
Purpose, Privilege, PresenceHi All,
I did a blog on the agency website last year and wanted to share it. Sometimes, I find, that giving a client a story, having it hanging in the waiting room, helps to get a sense of what we are doing in the ACT community. Please share as you need, it is basically a "witness" to the principles we live by in our clinical offices, schools and corporations. Peace
Questions on the hexaflex for young people
Questions on the hexaflex for young peopleThis handout can be used to generate discussion and introduce ACT processes. We use it with young people (teens) but it is also an easy introduction for adult clients. Adapted from earlier hexaflex question sheets, with simpler language (and pretty colours).
At-Risk Adolescents
At-Risk AdolescentsExperimental tests to date:
None Published
For further information contact: Amy Murrell or Kelly Wilson.
Author's note: We are posting this protocol in the hope that they will provide useful information in helping clients and spark further interest and research in ACT with children and adolescents. Please, recognize that we consider the treatment technology to be evolving in nature. These protocols, therefore, should be viewed as works in progress. The underlying principles should be adhered to, but the protocols can (and indeed should) be used with flexibility.
The protocol is attached to this page. Log into your ACBS member account to view/download the file.
Agoraphobia
AgoraphobiaAn ACT protocol designed for use with agoraphobia. Experimental tests to date: Hayes, S. C., Wilson, K. G., Afari, N., & McCurry, S. (November 1990). The use of Acceptance and Commitment therapy in the treatment of agoraphobia. Paper presented at meeting of the Association for the Advancement of Behavior Therapy, San Francisco. This is a very early anxiety protocol, written about 18 years ago. There has been a lot of work since on ACT for anxiety and though it is still recognizably the same kind of protocol, it has gotten better as we've gone along. For an excellent and detailed ACT anxiety protocol see the book by Eifert and Forsyth, 2005. Acceptance and Commitment Therapy for anxiety disorders. Oakland: New Harbinger. For further information contact: Steve Hayes (hayes@unr.edu), Department of Psychology, University of Nevada, Reno, NV 89557-0062.
"ACT For Life" - Group Intervention for Psychosis Manual
"ACT For Life" - Group Intervention for Psychosis ManualACT For Life Intervention
The intervention consists of four, two-hour weekly group sessions. The intervention is based principally around the “Passenger on the Bus” metaphor (Hayes, Strosahl, & Wilson, 1999), which is used to provide a consistent narrative thread throughout the groups. We use the metaphor to explore issues of workability, fusion, mindfulness, values and committed action in each of the sessions. We emphasise choice around participation, saying from the outset that, we would like people to participate as much as possible but it is an equally valid option to sit out of exercises. However, we generally find participants enjoy the interactive aspects of the group and often comment afterwards that the role playing is often one of the more memorable aspects of the group.
From the first group, we ask participants to be setting values goals that they can work towards throughout the week. However, we are careful to emphasise process goals here rather than outcome goals. As such, we frame this as an opportunity for participants to notice “passengers” or obstacles that arise as they approach the activity, and if the activity is completed, this is simply an added bonus.
We use PowerPoint presentations to make the groups more interactive and provide further structure to the groups. We have found this particularly useful in working with younger clients. The video vignette of the story of Tom can be downloaded from here: https://dl.dropbox.com/u/20036241/Tom_vignette_ACT_for_Life_groups.avi
The groups are designed to for approximately 8-10 participants. In each group we would have two to three therapists working with the group.
Each session follows a similar structure, which includes:
1. Warm-up exercise
2. Noticing (mindfulness exercise)
3. Discussion of the out of session activity from the previous week
4. Group discussion/ activity
5. Planning out of session activity
6 Session ACT Toolkit
6 Session ACT ToolkitThank you to everyone who has expressed interest in the toolkit. In order to effectively distribute the most up-to-date version of the toolkit, we have created a website for you and your clients to access:
The toolkit compiles information from around the web for psychoeducational and therapeutic use with clients. It also includes several exercises and worksheets designed by the creators. The website hosts the client version, and a Clinician Guide can be found here: http://www.helpwithact.com/toolkit
A training video of the creators reviewing the toolkit and how to use it can be accessed here: https://www.youtube.com/watch?v=Hu3f6UpUZJw
Please contact the creators with any questions or feedback.
ACT For Gambling Disorder
ACT For Gambling DisorderThis toolkit compiles information from around the web for psychoeducational and therapeutic use with clients. It also includes several exercises and worksheets designed by the creators. Please contact the creators with any questions or feedback.
The file can be accessed in its current form here:
https://docs.google.com/document/d/1hr3jsIE4RiiMPzY0EUIBxGyw-BwKI8r_pEcmmrALd7E/edit?usp=sharing
ACT For Grief (English Draft And Farsi Protocol)
ACT For Grief (English Draft And Farsi Protocol)ACT For Kids: Living a Valued Life
ACT For Kids: Living a Valued LifeThis ACT for Kids manual was developed by Steven Gordon, Michael Asher, and Michael Selbst.
Please note: due to copyright laws, ACBS removed images from the document. Therefore, some of the formatting might be slightly off.
ACT For Sleep Problems
ACT For Sleep ProblemsThis protocol was developed by Lindsay Fletcher at the University of Nevada, Reno. This protocol was developed by Lindsay Fletcher at the University of Nevada, Reno. Contact Lindsay for more information.
ACT Groups for Partial Hospitalization/Intensive Outpatient Programs (PHP/IOP)
ACT Groups for Partial Hospitalization/Intensive Outpatient Programs (PHP/IOP)I work in the Birches Program at the Brattleboro Retreat in Southern Vermont, a Partial Hospitalization/Intensive Outpatient Program (PHP/IOP). Participants usually stay in our program four to six weeks. I have developed a set of a dozen ACT-based groups that are inter-related and mutally supportive. Themes of: mindfulness; compassion; matrix; defusion; acceptance; anger; assertiveness; self-care; healthy relationships; finding motivation; values and action. Partcipants also have daily check-in groups that are more freely structured. I facilitate these themes on a rotating basis. I don't recommend them as stand-alone processes. I got most of the practices and metaphors from ACT trainings and books; if there is anything original, it's how I've sequenced things (and how I interact with the participants, with humor and on equal footing). I hope you will find these write-ups helpful.
Charlie Laurel, MS, LCMHC
ACT Made Simple: Togus One Week Protocol
ACT Made Simple: Togus One Week ProtocolAttached is a more developed version of the Togus one-week protocol. Kevin Polk presented the sketch of this at ACT SI III. Dr. Hambright has developed it further. Email Kevin if you have questions. polkkev@gmail.com.
Click here for the newest version of the protocol
Additional materials are routinely updated on Kevin Polk's blog
Noticing Hooks and What You Do Next
Noticing Hooks and What You Do Next
Togus Protocol 5/24/10
Togus Protocol 5/24/10Attached is a pdf of the latest 5-day (12 session) Togus PTSD Intensive Outpatient Program.
Email me with questions.
Kevin
Kevin Polk, Ph.D.
ACT ON HEALTH: An ACT group programme for weight management
ACT ON HEALTH: An ACT group programme for weight managementThis is a 6-session group programme designed for use in in a secure hospital setting, although the content could be used and adapted for other settings. It was written in response to the fact that many service users who are mandated to stay in hospital rapidly put on weight as a consequence of various factors including leading a sedentary lifestyle, prescribed medication, lack of control over hospital food choices, and comfort eating. Whilst there is often very good advice available about healthy eating and exercise, many service users seemingly choose not to follow this advice. We hypotheseised that this may be due to remoteness from values, and/or patterns of cognitive fusion and experiential avoidance. The resulting programme represents an attempt to draw attention to these processes in the service of making choices that were more mindful and more value-driven.
I would like to acknowledge the 'Obesity Stigma and Weight Management Acceptance and Commitment Therapy Treatment Manual', which is a one-day workshop protocol developed by Jason Lillis, Steven Hayes, and Kara Bunting. This is also available on the ACBS website and was a big part of the inspiration for our work.
Please contact Richard Bennett via info@thinkpsychology.co for more information.
ACT Self Help and the World Health Organization: "Doing What Matters in Times of Stress" and Self-Help Plus (SH+)
ACT Self Help and the World Health Organization: "Doing What Matters in Times of Stress" and Self-Help Plus (SH+)The World Health Organization (WHO) decided around 2015 to test ACT as a fully scalable psychological intervention. Dr. Mark van Ommeren, head of Mental Health, was looking for a radically transdiagnostic approach that could help with the wide variety of mental and behavioral consequences of war. The breadth of outcomes across different problems areas world wide for ACT attracted his attention. The war in the South Sudan was a particular issue at the time and Van Ommeren was aware that ACT had been deployed in Sierra Leone by the "Commit and ACT" clinic in Bo. ACT was proving helpful in the ebola outbreak there. Dr. Ommeren consulted with leaders of the ACT community (including Steve Hayes), asking for ideas of how best to simplify ACT and was referred to the work of Russ Harris. Van Ommeren was especially impressed with the simplicity of Russ Harris Illustrated Happiness Trap and Russ agreed to work with the WHO team to produce what became Doing What Matters in Times of Stress ("DWM"; 2020) -- an illustrated guide to ACT ideas stated in very non-technical language with graphical images.
WHO does not distribute health care advice until it is rigorously tested in a series of high quality randomized trials, beginning with very careful pilot work. These evaluation studies are deliberately conducted with developers held at arms length. If the methods are helpful they are then distributed for free. At the time, WHO had no fully scalable psychological interventions in its portfolio that could be distributed without the involvment of highly trained professionals. Over a period of 4-5 years ACT self-help was tested both in the simplest way (distributing the book, wih some minimal addition supports) and with the lessons in the book being described in audiotapes and discussed in a small group format by non-specialists in a program called "Self-Help +" ("SH+"; Brown et al., 2018; Tol et al., 2018).
ACT self-help successfully passed through these tests of efficacy across a range of settings, cultures, language communities, and problem areas. SH+ reduced anxiety and depression with war refugees at a level that was similar to self-help in economically privileged societies (Tol et al., 2020; Turrini et al., 2022), and reduced future development of mental health disorders by nearly by half over a year's time (Purgato et al., 2022). Importantly, increases in psychological flexibility were shown to mediate these changes (Lakin et al., 2023). Said simply, the evaluation studies suggested that ACT works and works via its putative processes of change.
Doing What Matters in Times of Stress is now distributed by WHO on a website that describes it in unusually broad terms: "Informed by evidence and extensive field testing, the guide is for anyone who experiences stress, wherever they live and whatever their circumstances." As an example of that view, when the COVID pandemic hit and WHO did not have an evidence-based approach for that problem, people were referred to that page https://www.who.int/publications/i/item/9789240003927 and studies were quickly conducted on DWM and SH+. The data showed that stressed health care workers were indeed helped (Riello et al., 2021; Mediavilla et al., 2023). Similarly WHO is now actively disseminating ACT self-help in the Ukraine to help with war survivors. Data are being collected there but it is not yet published.
ACT self-help is increasingly being built into the fabric of global health at WHO. In 2023 in an invited plenary talk at the World Congress of Cognitive and Behavioral Therapies in Seoul, Korea, WHO Mental Health head van Ommeren said that Doing What Matters in Times of Stress was now the most downloaded physical or mental health document of any kind at the World Health Organization.
SELF-HELP PLUS (SH+) (2021)
A group-based stress management course for adults (World Health Organization)
https://www.who.int/publications/i/item/9789240035119
Overview
Self-Help Plus (SH+) is WHO’s 5-session stress management course for large groups of up to 30 people. It is delivered by supervised, non-specialist facilitators who complete a short training course and use pre-recorded audio and an illustrated guide (Doing What Matters in Times of Stress) to teach stress management skills. The course is suitable for adults who experiences stress, wherever they live and whatever their circumstances. It has been shown to reduce psychological distress and prevent the onset of mental disorders. The format of SH+ makes it well-suited for use alongside other mental health interventions, as a first step in a step.
Available in English, Arabic, Juba Arabic, French, Portuguese, Spanish, Turkish, Ukrainian.
Doing What Matters in Times of Stress (2020)
An Illustrated Guide
https://www.who.int/publications/i/item/9789240003927
https://iris.who.int/handle/10665/331901
Overview
Doing What Matters in Times of Stress: An Illustrated Guide is a stress management guide for coping with adversity. The guide aims to equip people with practical skills to help cope with stress. A few minutes each day are enough to practice the self-help techniques. The guide can be used alone or with the accompanying audio exercises.
Informed by evidence and extensive field testing, the guide is for anyone who experiences stress, wherever they live and whatever their circumstances.
Available in Arabic, Armenian, Chinese, Czech, Dari, English, Estonian, Farsi/Persian, Finnish, French, German, Georgian, Greek, Hungarian, Indonesian, Italian, Japanese, Juba Arabic, Korean, Lithuanian, Malay, Polish, Portuguese, Romanian, Russian, Slovak, Spanish, Swedish, Tigrinya, Tongan, Turkish, Ukrainian, Urdu, Vietnamese.
How to Use WHO Self-help Plus Protocol
Webinar presented by Russ Harris and Claudette Foley
April 13, 2022
https://contextualscience.org/video/how_to_use_who_selfhelp_plus_protocol_webinar
Overview
This is a webinar on WHO's ACT protocol for refugees. We will answer Frequently Asked Questions about the protocol–also known as “Self-help Plus”-and explore how to implement it.
References:
Lakin, D. P., Cooper, S. E., Andersen, L., Brown, F. L., Augustinavicius, J. L. S., Carswell, K., Leku, M., Adaku, A., Au, T., Bryant, R., Garcia-Moreno, C., White, R. G., & Tol, W. A. (2023). Psychological flexibility in South Sudanese female refugees in Uganda as a mechanism for change within a guided self-help intervention. Journal of Consulting and Clinical Psychology, 91(1), 6–13. DOI: 10.1037/ccp0000774
Mediavilla, R., Felez-Nobrega, M., McGreevy, K. R., Monistrol-Mula, A., Bravo-Ortiz, M. F., Bayón, C., ... & Ayuso-Mateos, J. L. (2023). Effectiveness of a mental health stepped-care programme for healthcare workers with psychological distress in crisis settings: A multicentre randomised controlled trial. BMJ Mental Health, 26(1), 1-8. DOI: 10.1136/bmjment-2023-300697
Acarturk, C., Uygun, E., Ilkkursun, Z., et al. (2022). Effectiveness of a WHO self-help psychological intervention for preventing mental disorders among Syrian refugees in Turkey: A randomized controlled trial. World Psychiatry, 21, 88–95. DOI: 10.1002/wps.20939
Acarturk, C., Kurt, G., Ilkkursun, Z., Uygun, E., & Karaoglan-Kahilogullari, A. (2022). “Doing What Matters in Times of Stress” to decrease psychological distress during COVID-19: A randomised controlled pilot trial. Intervention, 20(2), 170-178. DOI: 10.4103/intv.intv_29_21
Turrini, G., Purgato, M., Tedeschi, F., Acartürk, C., Anttila, M., Au, T., et al. (2022). Long-term effectiveness of Self-Help Plus in refugees and asylum seekers resettled in Western Europe: 12-month outcomes of a randomised controlled trial. Epidemiology and Psychiatric Sciences, 31, E39. DOI: 10.1017/S2045796022000269
Purgato, M., Carswell, K., Tedeschi, F., Acarturk, C., Anttila, M., Au, T., Bajbouj, M., Baumgartner, J., Biondi, M., Churchill, R., Cuijpers, P., Koesters, M., Gastaldon, C., Ilkkursun, Z., Lantta, T., Nosè, M., Ostuzzi, G., Papola, D., Popa, M., Roselli, V., Sijbrandij, M., Tarsitani, L., Turrini, G., Välimäki, M., Walker, L., Wancata, J., Zanini, E., White, R., van Ommeren, M., & Barbui, C. (2021). Effectiveness of Self-Help Plus in preventing mental disorders in refugees and asylum seekers in Western Europe: A multinational randomized controlled trial. Psychotherapy and Psychosomatics, 90, 403–414. DOI: 10.1159/000517504
Riello, M., Purgato, M., Bove, C., Tedeschi, F., MacTaggart, D., Barbui. C., & Rusconi, E. (2021). Effectiveness of self-help plus (SH+) in reducing anxiety and post-traumatic symptomatology among care home workers during the COVID-19 pandemic: A randomized controlled trial. Royal Society of Open Science, 8, 210219. DOI: 10.1098/rsos.210219
Tol, W.A., Leku, M.R., Lakin, D.P., Carswell, K., Augustinavicius, J., Adaku, A., Au, T.M., Brown, F.L., Bryant, R.A., Garcia-Moreno, C., Musci, R.J., Ventevogel, P., White, R.G., van Ommeren, M. (2020) Guided self-help to reduce psychological distress in South Sudanese female refugees in Uganda: a cluster randomised trial. Lancet Global Health, 8(2), e254–63. DOI: 10.1016/S2214-109X(19)30504-2
Tol, W. A., Augustinavicius, J., Carswell, K. Adaku, A. M., Leku, R., Brown, F. L., Garcia-Moreno, C., Ventevogel, P., White, R. G., Kogan, C.S., Bryant, R. and van Ommeren, M. (2018). Feasibility of a guided self-help intervention to reduce psychological distress in South Sudanese refugee women in Uganda. World Psychiatry, 17(2), 234-235. DOI: 10.1002/wps.20537
Tol, W. A., Augustinavicius, J., Carswell, K., Brown, F. L., Adaku, A. M., Leku, R., Garcia-Moreno, C., Ventevogel, P., White, R. G. and van Ommeren, M. (2018). Translation, adaptation, and pilot of a guided self-help intervention to reduce psychological distress in South Sudanese refugees in Uganda. Global Mental Health. DOI: 10.1017/gmh.2018.14
Brown, F. L., Carswell, K., Augustinavicius, J., Adaku, A., Leku, M. R., White, R. G., Ventevogel, P., Kogan, C. S., García-Moreno, C., Bryant, R. A., Musci, R. J., van Ommeren, M., & Tol, W. A. (2018). Self Help Plus: study protocol for a cluster-randomised controlled trial of guided self-help with South Sudanese refugee women in Uganda. Global mental health, 5, e27. DOI: 10.1017/gmh.2018.17
Epping-Jordan, J., Harris, R., Brown,F.L., Carswell, K., Foley, C., García-Moreno, C., Kogan, C., & van Ommeren, M. (2016). Self-Help Plus (SH+): a new WHO stress management package. World Psychiatry, 15, 295-296. DOI: 10.1002/wps.20355
ACT Treatment Outlines for Anxiety and Depression (Forman et al., 2007 effectiveness study)
ACT Treatment Outlines for Anxiety and Depression (Forman et al., 2007 effectiveness study)This page includes treatment outlines that were used in the Forman and colleagues (2007) effectiveness study comparing ACT and CT for anxiety and depression.
Please note (From Sue Orsillo): The research manual referenced in the Anxiety Outline attached below is no longer distributed since the publication of the book Mindfulness and Acceptance-based Behavioral Therapies in Practice. The book is intended to serve as a "clinical manual". The research protocol was an in-house protocol that states which questionnaires should be handed out in each session for the study, etc. That manual assumes the reader was trained by, and is supervised by, us. It is not written in a way that is easily useable by others.
Experimental tests to date:
Forman, E. M., Herbert, J. D., Moitra, E., Yeomans, P. D., & Geller, P. A. (2007). A randomized controlled effectiveness trial of Acceptance and Commitment Therapy and Cognitive Therapy for anxiety and depression. Behavior Modification, 31(6), 772-799.
ACT for Anger Group
ACT for Anger GroupWe created this 8-week group as part of our postdoctoral residency program development project at Kaiser Permanente in Vallejo, CA.
Megan Foret, Psy.D. and Patricia Eaton, Psy.D.
Note: Much of the content ideas can be credited to other authors who are acknowledged on page two.
ACT for Athletes (The Flexible Mind)
ACT for Athletes (The Flexible Mind)'The Flexible Mind - Session Guides' are intended for use by practitioners working with athletes who wish to use Acceptance and Commitment Training to support the performance and mental health of the athletes. The sessions are organized as follows:
- Introducing Athletes to The Flexible Mind approach (Session 1)
- Mind full vs. Mindful (Session 2)
- Orientating to Our Inner Compass (Session 3)
- Being Open, Living Big (Session 4)
- Getting Present with the Discomfort (Session 5)
- Flexibility… of the Psychological Kind (Session 6)
- Developing the Game Plan (Session 7)
For further details please see: www.FlexibleMind.co.uk and the book: http://cutt.ly/CbM2bV4 Twitter: @Mind_Flexer
We hope that the materials are helpful. If you have any queries or feedback please contact Ross White (admin@strive2thrive.co.uk).
ACT for Depression and Anxiety Group - Cornell University Counseling and Psychological Services
ACT for Depression and Anxiety Group - Cornell University Counseling and Psychological ServicesIntroduction - These materials accompany the ACT for Depression and Anxiety Group...
These materials accompany the ACT for Depression and Anxiety Group developed by Matt Boone at Cornell University's Counseling and Psychological Services. It is a 10 session college counseling center group which combines didactic elements, mindfulness exercises, experiential exercises, group discussion/process, and homework (called LIFE Exercises). The protocol described here is very close (about 90%) to what was used in Matt Boone's pilot study of a transdiagnostic ACT group in college counseling. A few homework worksheets have been removed to give participants less to do between sessions, and the order of a some elements have been changed slightly.
The group is meant to fit within a single semester. The first half of the semester covers the six processes of psychological flexibility. The second half focuses on mobilizing psychological flexibility in the service of values-driven committed action – both inside the group, as members interact with one another, and outside the group in the students' lives. The second half looks a little bit more like traditional group therapy – group leaders are encouraged to incorporate the interpersonal group process into conversations about acceptance, mindfulness, and values.
The materials were collated and revised by Matt Boone and Cory Myler during the 2011-2012 academic year. Feel free to contact either Matt or Cory about any aspect of the group. Matt can be reached at matthewsboone@gmail.com. Cory can be reached at cory.myler@gmail.com.
Group Format
Each group meeting is organized roughly as follows:
● opening mindfulness exercise
● review of LIFE Exercises from the previous week
● didactic portion with group discussion
● experiential exercise with group discussion
● further group discussion
● assigning LIFE exercises for next time
The didactic portion ends in the fifth session and is reinforced by the readings.
The progression of the group throughout the semester is roughly organized around the six processes of psychological flexibility. These are defusion, acceptance/willingness, contact with the present moment, self as context (called the "observing self" in the group), values, and committed action.
The order is as follows:
● session 1: "control is the problem" and contact with the present moment
● session 2: defusion
● session 3: acceptance/willingness
● session 4: values
● session 5: observing self
● session 6: committed action
● session 7-10: all processes, with a focus on building greater patterns of committed action in the service of values
Background
It is helpful if you have been to at least one ACT training and you are familiar with some core ACT texts. At minimum you should read ACT Made Simple, because many of the group's didactic elements are drawn from it, and The Happiness Trap, because readings from it are used as homework. Other good texts are The Mindfulness and Acceptance Workbook for Depression, Learning ACT, Mindfulness for Two, Get Out of Your Mind and Into Your Life, Acceptance and Commitment Therapy: The Process and Practice of Mindful Change, and The Mindfulness and Acceptance Workbook for Anxiety. All of these influenced the creation of the group. Full citations of these texts are included at the end of this document..
Session Outlines
Outlines for each group session are included. For the first five sessions, the outlines give instructions which accompany the PowerPoint slides. The outlines are far more detailed in the first few sessions, mostly because the majority of the psychoeducation happens then, but partly because limitations on time and resources have prevented writing everything out extensively. You should use your best judgment and your experience with leading groups, but feel free to contact Cory or Matt with questions.
Power Points
As noted above, PowerPoint is used to introduce didactic elements in the first five sessions. Beware of relying on them too much. Remember: ACT draws on metaphors and experiential exercises just as much as it relies on education. Most of the text in the PowerPoints comes directly from ACT texts. Citations are included where appropriate, but some may have been forgotten. The pictures are all from Google images, and their copyright is uncertain.
Readings
The readings are not included. Group members should be encouraged to buy The Happiness Trap, and the short excerpt from the Mindfulness and Acceptance Workbook for Depression assigned in session 3 can be photocopied and passed out. Optional additional readings are also excerpted from The Acceptance and Mindfulness Workbook for Depression. If you assign the optional readings, consider encouraging students to buy the book. These readings expand on the concept of defusion. The Acceptance and Mindfulness Workbook for Depression extensively explores defusion, the function of thinking, and potential pitfalls in getting wrapped up in the mind.
Worksheets and Handouts
Most worksheets and handouts are adapted from ACT Made Simple and The Happiness Trap. Every attempt has been made to cite original sources where appropriate. The excerpt from The Acceptance and Mindfulness Workbook for Depression includes a worksheet which is completed for homework between sessions 3 and 4.
Mindfulness MP3s
Four mindfulness exercises that are used for homework are included in MP3 form. Some of them are also used as exercises to mark the beginning of group sessions. (However, group leaders are encouraged to lead the exercises themselves rather than playing the MP3s in group.) Because the recordings were created in an amateur home studio, they sound fine through speakers, but there is some background noise when you listen to them on headphones. They are designed to be short because busy students often will not do lengthy mindfulness exercises for homework. Keeping them short hopefully makes it more likely that they will do them.
Scripts for all of them except "Brief Mindfulness" can be found in the ACT literature. The script for "Brief Mindfulness" was improvised by Matt Boone, but it's very close to other short mindfulness exercises in the literature. It is meant as a brief instruction on mindfulness, as well as a mindfulness exercise in itself. The scripts for "Leaves on a Stream" and "Acceptance of Thoughts and Feelings" are taken from the Mindfulness and Acceptance Workbook for Anxiety. Both can also be found in Acceptance and Commitment Therapy for Anxiety Disorders and "Leaves on a Stream" can be found in many other ACT texts. "Willingness Exercise" is an extensive acceptance exercise taken from ACT Made Simple. (It is similar to "physicalizing" in the ACT literature. It is assigned for homework a number of times throughout the group to facilitate exposure to feared internal stimuli like thoughts and feelings. Scripts for some of the other group's mindfulness exercises are included with these materials. They are similar to mindfulness exercises found in the ACT literature.
Experiential Exercises
Detailed instructions for many experiential exercises are included, but some are not. For example, nothing is written about "Eyes On," but there is information about it in many ACT texts. The same goes for "Take Your Mind for a Walk."
Notes to Group Leaders
● Be flexible. Feel free to jettison the psychoeducation or any experiential exercise if it does not feel appropriate for a particular group session. The most important thing is that participants get to encounter and understand, both experientially and intellectually, what psychological flexibility is like. Too much structure can get in the way of the group process.
● Working in the "here and now." Despite the psychoeducation elements, some really powerful "here and now" work can be done in this group if there is space left open for it. The ACT vocabulary gives students a way to talk about what they're experiencing in the moment and helps group members understand their reactions as part of their histories, not what others are "doing" to them. Doing this work is not really covered in these materials – draw on your training in group therapy. If you need further reading, see the chapter below, and especially consult Yalom's seminal work, The Theory and Practice of Group Psychotherapy.
● The book chapter "Acceptance and Commitment Therapy (ACT) in Groups" is included as optional reading for group facilitators. It presumes the reader has already had an introduction to the six processes of psychological flexibility.
● Please feel free to e-mail Matt or Cory with any questions.
Cheers!
Resources
Boone, M. S., & Manning, J. (2012). A pilot study of an Acceptance and Commitment Therapy group for anxiety and depression in a college counseling center. Manuscript in preparation.
Boone, M. S. , & Canicci, J. (In press). Acceptance and commitment therapy (act) in group. In Pistorello, J. (Ed.). Mindfulness and Acceptance on the College Campus. Oakland, CA: New Harbinger.
Luoma, J., Hayes, S. C., & Walser, R. (2007). Learning ACT. Oakland, CA: New Harbinger.
Eifert, G. H., & Forsyth, J. P. (2005). Acceptance and commitment therapy for anxiety disorders: a practitioner's treatment guide to using mindfulness, acceptance, and values-based behavior change strategies. Oakland, CA: New Harbinger.
Forsyth, J. P., &, Eifert, G. H. (2007). The mindfulness and acceptance workbook for anxiety. Oakland, CA: New Harbinger.
Harris, R. (2010). ACT made simple. Oakland, CA: New Harbinger.
Harris, R. (2008). The happiness trap. Boston, Massachusetts: Shambhala.
Hayes, S. C., & Smith, S. (2005). Get out of your mind and your life: The new acceptance and commitment therapy. Oakland, CA: New Harbinger.
Hayes, S. C., Strosahl, K., & Wilson, K. G. (2011). Acceptance and commitment therapy: The process and practice of mindful change (2nd edition). New York: Guilford Press.
Strosahl, K., & Robinson, P. (2007). The mindfulness and acceptance workbook for depression. Oakland, CA: New Harbinger.
Walser, R. D., & Pistorello, J. (2004). ACT in group format. In S. C. Hayes & K. D. Strosahl (Eds.), A practical guide to acceptance and commitment therapy (pp. 347-372). New York: Springer.
Yalom, I. (2005). The theory and practice of group psychotherapy (5th ed.). New York: Basic Books.
ACT for HIV-related Stigma and Shame
ACT for HIV-related Stigma and ShameThe case study this protocol resulted in is not yet in print, though a description and theoretical elaboration will be presented in:
Skinta, M.D. (n.d.). Acceptance and compassion-based approaches for invisible shame: Working with sexual minorities and chronic illness. In A. Masuda (Ed.), Cultural issues in acceptance and mindfulness-based approaches. Oakland: New Harbinger Publications. In press (anticipated Spring 2014).
As noted in the front matter, this manual was largely drawn from existing protocols and adapted for a focus on HIV. By drawn from, I mean cut-and-paste was widely used, with revisions made for content, as this originally was intended as only a conversation piece between the co-therapists. Given the number of requests backchannel in the year since, however, it seems it may be useful to share in this forum. For this reason, the manual content itself should not be considered original work of Skinta or Wells, but rather an adoption of both the Self-Stigma and Shame in Substance Addictions Manual on this page, as well as Eifert and Forsyth's ACT for Anxiety Disorders and Dahl et al's The Art and Science of Valuing in Psychotherapy.
Even within our pilot, this was an evolving work, with different techniques explored and shared. For further information, or excited and lively conversation about working with HIV-affected communities with ACT, please contact Matthew Skinta.
Farsi/Persian version of the file adopted for Iranian Population - راهنمای درمان گزوهی پذیزش و تعهد (ACT)بزای کاهش شزم مبتلایان به HIV مثبت
Farsi/Persian version of the file adopted for Iranian Population - راهنمای درمان گزوهی پذیزش و تعهد (ACT)بزای کاهش شزم مبتلایان به HIV مثبتراهنمای درمان گزوهی پذیزش و تعهد (ACT)بزای کاهش شزم مبتلایان به HIV مثبت
ACT for Irritable Bowel Syndrome
ACT for Irritable Bowel SyndromeThis is a protocol created by Nuno Ferreira and David Gillanders for the use of ACT with Irritable Bowel Syndrome (IBS).
This protocol was used for a single group session that was then followed by work with a self-help workbook.
In the attachments you will find all the steps used during the session. The session maps on the contents of the self-help book and it is best used in conjunction with this book. You will also find the forms we used during the workshops to facilitate some of the exercises.
The effectiveness of this protocol was tested with refractory IBS patients (patients who had had a minimum of 12 months input from a physician without any significant change). Study participants showed improvement in symptoms, quality of life, use of avoidant behaviours and gastrointestinal specific anxiety after the intervention. The effects were medium to large and held up at 6 month follow-up. A paper regarding this study is due to be published soon.
The self-help workbook ("Better living with IBS") is now comercially available through Exisle Publishers or for those in the UK through Sheldon Press.
We'll be happy to respond to questions regarding this protocol.
Best,
Nuno Ferreira
Teaching Fellow in Clinical Psychology
University of Edinburgh
ACT for Parents of Anxious Children (ACT-PAC) Manual by Lisa Coyne & Phoebe Moore
ACT for Parents of Anxious Children (ACT-PAC) Manual by Lisa Coyne & Phoebe MooreThe ACT-PAC manual is a 6 session manual for parents of children with anxiety. Five of the sessions are for general use, and the remaining module targets parent behaviors emblematic of families of anxious children. The manual was written so that clinicians new to ACT could deliver it word-for-word if they wish; however, it also integrates options for choosing different but functionally equivalent exercises and activities. It is a principles-based manual, and we offer it to our ACBS community in the spirit of open science, to disseminate, share, research, adapt, and improve by our peers who will continue this work. Please do cite us where appropriate. Other than that, please help yourselves to this resource. May we help to support many families who are struggling. -Lisa & Phoebe
ACT for Parents of Developmentally Disabled Children Manual
ACT for Parents of Developmentally Disabled Children ManualA manual for delivering ACT to parents, targetting parenting stress. This manual was written specifically for parents of children with developmental disabilities, however, it could be adapted for use with other high-risk parents. The intervention is written as a four hour intervention with two sessions of two hours each. This intervention was found to be effective when used in conjunction with Stepping Stones Triple P with families of children with Cerebral Palsy and families of children with Acquired Brain Injury. In the RCT of Stepping Stones Triple P and Acceptance and Commitment Therapy, Acceptance and Commitment Therapy was found to have a beneficial effect, above and beyond conventional parenting interventions.
Relevant Publications
Whittingham, K., Sanders, M., McKinlay, L. & Boyd, R.N. (2014). Interventions to Reduce Behavioral Problems in Children with Cerebral Palsy: An RCT. Pediatrics. Accepted 14/02/2014 Epub ahead of print.
Brown, F., Whittingham, K., Boyd R., McKinlay, L. & Sofronoff, K. (in press)
Improving child and parenting outcomes following paediatric acquired brain injury: A randomised controlled trial of Stepping Stones Triple P plus Acceptance and Commitment Therapy. Journal of Child Psychology and Psychiatry. Accepted 27/01/2014.
Whittingham, K., Sanders, M.R., McKinlay, L. & Boyd, R.N. (2013) Stepping Stones Triple P and Acceptance and Commitment Therapy for parents of childrenwith cerebral palsy: Trial protocol. Brain Impairment. 14 (2), 270-280.
Brown, F., Whittingham, K., McKinlay, L., Boyd, R.N. & Sofronoff, K. (2013) Efficacy of Stepping Stones Triple P plus a stress management adjunct for parents of children with acquired brain injury: The protocol of a randomized
controlled trial. Brain Impairment. 14 (2), 253-269.
ACT for Perinatal Mood and Anxiety Disorders Skills Group Handouts
ACT for Perinatal Mood and Anxiety Disorders Skills Group HandoutsAttached are ACT skills group handouts that we have used on our perinatal psychiatry inpatient unit at UNC Hospital at the University of North Carolina at Chapel Hill. They were adapted from multiple other sources, so the content is in no way original. Also attached is our manuscript describing the rationale and use of these materials.
For additional information, you can contact Crystal Schiller at crystal_schiller@med.unc.edu.
ACT for Psychosis Recharged
ACT for Psychosis Recharged RCTingeyACT for Psychosis Treatment Protocol
ACT for Psychosis Treatment ProtocolACT for outpatient adolescent substance treatment
ACT for outpatient adolescent substance treatmentThis manual provides guidance for outpatient individual and family sessions for adolescents with co-occurring psychiatric and substance use disorders. The model includes motivational interviewing, acceptance and committment therapy, and contingency managment. Preliminary data has been published in the Journal of Contextual Behavioral Science 107;6:375-379.
Please provide feedback on www.DrThurstone.com.
ACT group "ACT on Goals" protocol for Chronic Physical Conditions, and / or Persistent Pain (and Mental Health Issues) 2018 version, previously called More to Life
ACT group "ACT on Goals" protocol for Chronic Physical Conditions, and / or Persistent Pain (and Mental Health Issues) 2018 version, previously called More to LifeMore to Life - Comment submitted by kaileen on May 20, 2018 - 5:52pm.
This group course has been run 19 times (and more possibly more overseas) by psychologists, social workers and occupational therapists, with good outcomes. Recently I've rewritten it slightly to include bit more on persistent pain and called it 'ACT on Goals'. Email me if you want a copy.
ACT on Your Recovery - 15 session Substance Misuse Group Manual
ACT on Your Recovery - 15 session Substance Misuse Group ManualThis is a 15 session ACT group manual for substance use issues that I've run in some UK treatment services. The manual provides a general structure for introducing ACT exercises and other addiction related treatment components (e.g., skills training), though we've always emphasised flexibility in delivery, and never slavishly following the manual.
This group was designed as a modular structure: Three modules of five sessions each, with a predominant focus on OPEN, ACTIVE, and AWARE.
I hope it's of use to people.
all the best
Lee Woodward
Acceptance and Commitment Training for Substance Abuse Counselors
Acceptance and Commitment Training for Substance Abuse CounselorsAcceptance and Commitment Training for Substance Abuse Counselors protocol.
Experimental tests to date:
Varra, A. A., Hayes, S. C., Roget, N., & Fisher, G. (2008). A randomized control trial examining the effect of acceptance and commitment training on clinician willingness to Use evidence-based pharmacotherapy. Journal of Consulting and Clinical Psychology, 76, 449-458.
Acceptance-Based Treatment for Eating Disorders
Acceptance-Based Treatment for Eating DisordersThis treatment consists of eight biweekly 75-minute sessions conducted in group format, intended for use at a residential treeatment facility.
Preliminary empirical support for this manual is published under:
Juarascio, A., Shaw, J., Forman, E. M., Timko, C. A., Herbert, J. D., Butryn, M. L., & Lowe, M. (2013). Acceptance and Commitment Therapy for eating disorders: Clinical applications of a group treatment. Journal of Contextual Behavioral Science, 2, 85-94.
Anger Group Outline - ACT Based
Anger Group Outline - ACT BasedThis is an outline of a 7-week group on Dealing with Anger using an ACT framework. The outline includes both facilitator notes, as well as client handouts. We used the materials with a group of adult clients referred from a local community mental health agency, and the clients responded well to the materials and the group process that resulted. Psychology graduate students were the main group facilitators, with a psychologist supervising their work. Feel free to use/adapt the materials.
Annette Dufresne, Ph.D., C.Psych.
Ontario, Canada
dradufresne@gmail.com
BEACHeS: Brief Engagement and Acceptance Coaching in Hospice Settings
BEACHeS: Brief Engagement and Acceptance Coaching in Hospice SettingsThis is the intervention manual used in the BEACHeS Study. The study was a single case experimental design, testing the feasibility and acceptability of a brief individual delivered, manualised ACT intervention to people who recently transitioned into receiving specialist palliative care services. All patients had a cancer diagnosis, which was considered non-curable.
You can read more about the research in the attached paper.
Hulbert-Williams, N. J., Norwood, S. F., Gillanders, D., Finucane, A. M., Spiller, J., Strachan, J., … Swash, B. (2021). Brief Engagement and Acceptance Coaching for Hospice Settings (the BEACHeS study): results from a Phase I study of acceptability and initial effectiveness in people with non-curative cancer. BMC Palliative Care, 20(1), 1–13. https://doi.org/10.1186/s12904-021-00801-7
The manual contains details of expected training to be able to deliver the intervention safely and effectively, and a disclaimer as follows:
DISCLAIMER
This manual has been written and provided in good faith by the BEACHeS Research Team. The manual and intervention has not been the subject of any patient complaint or adverse event in the BEACHeS research study. The BEACHeS study team, Marie Curie, The University of Chester or The University of Edinburgh accept no liability or responsibility for any subsequent use of this intervention in other settings. Individuals and services using this manual take responsibility for doing so, and for ensuring practitioners using this intervention are well trained, supported and supervised, and are competent and legal to deliver services within the country in which they are working.
The intervention was also supported by audio files that can be given to participants which can be accessed here
Better Living with Illness
Better Living with IllnessWe are very excited to share this protocol with the ACT community! The Better Living with Illness group is an ACT intervention designed for people living with chronic physical illness, to be run over 6 weeks, with 2 follow-up sessions 1 and 3 months post-intervention. Sessions last 2.5 hours, including a half-hour break in the middle.
This protocol is based on others published here (e.g. chronic pain), but also has some additional elements included that are relevant to this group, such as pacing, assertive communication, goal setting and problem solving skills, delivered in an ACT-consistent way. Its also novel in its transdiagnostic approach: this group was designed to bring people living with different long term physical health conditions together, acknowledging that commonalities that exist across many diagnoses (both physical and mental).
The group has been run in NHS Fife, Scotland for just over 2 years, in a repeated measures controlled trial in conjunction with the University of Edinburgh for a DClinPsy thesis. For the evaluation, we defined chronic physical illness as conditions that had lasted for a minimum of 12 months and required some form of management (e.g. medication). We had 33 participants complete. The results (n=33 for completers) indicated significant improvements in HADS scores compared to the baseline control period, with similar improvements in measures of valued living (Matthew Smout's VQ measure) and psychological flexibility (AAQ-II). This was in the context of no significant change on perceived health status. These processes were also found to mediate change in HADS scores. We will shortly be submitting a paper for publication on this and will update here with details.
Overall, participants were very positive about the group and their experiences in it, and really valued it.
Please do get in touch if you'd like to know a bit more about this group.
And if you do download and use the protocol, please get in touch with David Gillanders to let him know - david.gillanders@ed.ac.uk
Linsay Brassington linsaybrassington@hotmail.com
Co-authors:
Nuno Ferreira, University of Edinburgh
Shona Yates, NHS Fife
Jackie Fearn, NHS Fife
Pam Lanza, NHS Fife
Kim Kemp, NHS GGC
Hannah Dale, NHS Fife
Mandy Forbes, NHS Tayside
David Gillanders, University of Edinburgh
Publication of the BLI results - Comment submitted by David Gillanders on May 24, 2018
The journal article that describes the research and evaluation of the Better Living with Illness Protocol in NHS Fife, by the team named above can be found here:
Brassington, L., Ferreira, N. B., Yates, S., Fearn, J., Lanza, P., Kemp, K., & Gillanders, D. (2016). Better living with illness: A transdiagnostic acceptance and commitment therapy group intervention for chronic physical illness. Journal of Contextual Behavioral Science, 5(4), 208–214. http://doi.org/10.1016/j.jcbs.2016.09.001
https://www.sciencedirect.com/science/article/pii/S2212144716300576?via%3Dihub
Using the Better Living with Illness Protocol in Neurological Populations
Using the Better Living with Illness Protocol in Neurological PopulationsThe Department of Neuropsychology at the James Cook University Hospital in Middelsborough U.K. has adapted the BLI protocol and has been using it with people with a variety of neurological conditions and impairments. They have published a preliminary report on the adaptation and outcomes with a small series of cases. That can be seen in:
Hill, G., Hynd, N., Wheeler, M., Tarran-Jones, A., Carrabine, H., & Evans, S. (2017). Living well with neurological conditions: Evaluation of an ACT-informed group intervention for psychological adjustment in outpatients with neurological problems. The Neuropsychologist, 3, 58 – 63.
A summary of the data and the article itself are available as attachments to this page.
Dr Hill has also produced an audio recording of the exercises they use in this group and has made these available for free download below in the zip file. These are made available for non commerical use.
For more information about the adaptations, contact:
Dr. Geoff Hill
Clinical Psychologist in Neuropsychology
Department of Neuropsychology
Disability Services Centre
James Cook University Hospital
Marton Road
Middlesbrough
TS4 3BW
Geoffrey.Hill@stees.nhs.uk
Choice Point Model
Choice Point ModelFrom Joseph Ciarrochi:
I wanted to introduce you to a model Ann Bailey, Russ Harris, and I have come up with for facilitating ACT and CBS interventions. The three of us have been using this model continuously, now, for about 6 months, with a wide variety of clients, and we are finding it to be extremely effective. Clients love it.
You can find a PDF of the powerpoint on the Choice Point Model below.
You can also find the powerpoint below, along with an example worksheet.
A choice point is a moment in time when it is possible to choose between values consistent and values inconsistent behaviour.The CP allows you to record key aspects of the situation, the difficult inner experience that shows up, the values ,skills, and strengths used to respond effectively to the situation and the inner experience, and finally the behaviour that can be either value consistent or value inconsistent.
What is the choice point model
The Choice Point is a simple way to help you and your client keep track of where you are in an ACT/ACBS intervention. In the above document,we show how you can use it to summarise willingness, defusion, and self-compassion. It can be used to keep track of all ACT processes, as Russ will illustrate later in videos. We have found that Choice Point gives the client a sense of a safe framework and allows them to be more exploratory, knowing that they can always come back to the ³map², the CP, and know where they are.
There will be questions about how this model relates to other models. The choice point has a clear mapping to tobias and Joanne¹s Bulleseye ,in that the emphasis is on value consistency, rather than appetitive versus aversive-driven behaviour. It is also inspired by the Matrix ability to put things into a simple framework and reach many people .We were struggling to do just that, as we (Ann and I) had to teach ACT principles to dieticians, football players, and other folks who did not necessarily have sophisticated psychological training. After much trial and error with clients, we finally got to the Choice point (and Ann had been using a variant of this for years with Borderline clients).
As far as we can tell, the choice point complements other approaches and does not contradict them.
The Choice Point model illustrates different points of intervention. For example, for the ³situation² part of the choice point (bottom), one can target situation selection and modification (e.g., problem solving, re-engineering the environment). In the values and skills section (bottom right), you can help the client to modify the form or frequency of inner experience (traditional CBT) or you can help the client to respond flexibly to the situation and the inner experience (ACT) or you can help the client identify and use strengths (positive psychology). Of course most therapies probably do all of these activities and differ only in emphasis.
The choice point model and contextual behavioural science: Going beyond ACT
We have attempted to make the CP more generally about Contextual Behavioral Science than ACT. Thus, the choice point worksheet has a place to describe the situation (antecedent events) and the consequences (whether the behaviour is value consistent or inconsistent). The Choice point allows for some avoidance behaviour to be a value-consistent and some appetitive behaviour to be value inconsistent . In a CBS approach, no behaviour is inherently good or bad. It is always assessed in the context of the situation and its consequences to the organism. I have long argued that some appetitive behaviour is value-inconsistent. It doesn¹t have to be "crazy-appetitive" as Kelly puts it. It can be a series of small choices, small appetitive moves, that gradually take you away from the things you
care about. For example, a recent paper shows that induced positive mood can lead to overeating. That sounds like eating under mild appetitive control. Other research shows that as the number of people you eat with increases, so does the amount you eat again, I doubt this effect is mainly about avoidance.
OK, let me be controversial here (you all know how much a love this community and my belief that controversy is necessary). I think that we in ACT (including me) are sometimes making three mistakes.
Mistake 1: Its all about avoidance. I don¹t think we should assume avoidance underpins all unhelpful behaviour. The psychodymanic folks have tried that before us, and I think mostly failed. You can always play the game of "gotcha" and come up with an avoidance explanation for anything, but I think it would be fairly surprising if the appetitive system did not play a key role in some value-inconsistent behaviour. Mostly, behaviour is under both appetitive and aversive control (e.g., I feel guilty if I don¹t exercise and I love exercising)
I'm not saying that avoidance is not central to our suffering; I'm just saying that a complete CBS approach will include potential causes of unworkable behaviour, other than what is explicitly stated in ACT hexeflex.
Mistake 2: Mindfulness is universally good and the "holy grail" of well-being. Being mindful is just another behaviour, which means it's utility needs to be evaluated in context. Recent research suggests that
mindfulness not only disrupts bad habits, it can slow the formation of good habits. Of course, everything depends on how you define the behaviour "mindfulness" and we could play the game of "gotcha," where anything beneficial can be described as involving mindfulness. If everything beneficial is based on mindfulness, then I propose we replace the word "mindful" with "beneficial." I do prefer the ACT phrase, "contact with the present moment", as it seems to have less baggage, and one can easily imagine when contact with the present moment isn't the best move (e.g., when planning and imagining possible futures).
Mistake 3: All attempts at reappraisal and suppression are bad. Again, I return to the CBS mantra the attempt to change inner experience is a type of behaviour, that can only be evaluated in context. I think the coming years will see a push to more clearly specify when interventions like cognitive reappraisal are most and least likely to work (a recent study suggests reappraisal does not work so well when folks can control the situation). Anyway, as you folks know, ACT already does plenty of cognitive restructuring types of stuff, in the form of psych-education and in expanding how people think about feared things.
In closing, I hope what I am putting out there will be of use.
ACT WITH CHOICE MODEL
ACT WITH CHOICE MODELThis variation on the Choice Point model provides an explanatory top sheet and a worksheet to identify the difference between working in the "Grey" and working in the "Green". You can access our other ACT, CFT and CBT resources by visiting http://www.thinkcbt.com and following the free downloads button. Please contact me on admin@thinkcbt.com if you want to publish free ACT resources on our pages.
Adaptation of Choice Point Handout
Adaptation of Choice Point HandoutI did a Visio version of the choice point handout and I am attaching it here in case others find it useful.
I added in the automatic reaction being triggered step as I find it helpful for a discussion about how our habitual reactions are so fast they have begun their reactions before we are consciously aware of them. So we are making our choice to move towards what's important in the face of habitual reactions that are often already avoidantly moving us away.
Thanks to the originators of this really helpful handout.
Choice Point Español
Choice Point EspañolSubmitted to the ACBS ACT for Professionals listserv by Daniel Granados-Salazar on December 4, 2021
Hi all!
I did this worksheet that sometimes I use with clients. Maybe someone can find it useful for clients too. It is in Spanish. It is inspired from the Choice Point by Russ Harris and a modified version Lou Lasprugato gave us in a workshop. I am very grateful with both of them.
I hope it helps!
Warmly,
Daniel
¡Hola a todos!
Hice esta hoja de trabajo que a veces uso con los clientes. Quizás alguien pueda encontrarlo útil para sus clientes también. Está en español. Está inspirado en el Choice Point de Russ Harris y una versión modificada que Lou Lasprugato nos dio en un taller. Estoy muy agradecido con ambos.
¡Espero que sea de utilidad!
Abrazo.
Daniel
Choice Point Russian
Choice Point Russian CommunityChoice point for young people
Choice point for young peoplePlease see the main Choice Point page for a full description of the concept of this tool. This is merely a more young-person friendly version, with some consistency with the DNA-V model. I drew this and created a PDF so that I could upload it but I find the best way to use this is to draw it with clients, rather than print out the worksheet. This is well and truly work in progress so any feedback would be much appreciated!
Surfing Your Stress To Success: Kevin Polk's iView Videos
Surfing Your Stress To Success: Kevin Polk's iView VideosThese two videos give the audience a taste of how to approach using the iView -- or finding the place from which we notice all things (moving toward values and moving away from unwanted private experiences).
Contact Kevin for additional information.
Chronic Pain Treatment Protocol
Chronic Pain Treatment ProtocolAn eight session protocol for chronic pain intended for use in outpatient settings. Includes preface, therapist guide, patient manual, and references.
Experimental tests to date:
Vowles, K. E., Wetherell, J. L., & Sorrell, J. T. (2009). Targeting acceptance, mindfulness, and values-based action in chronic pain: Findings of two preliminary trials of an outpatient group-based intervention. Cognitive and Behavioral Practice, 16, 49-58.
Chronic Pain-Group Treatment Facilitator and Patient Manual
Chronic Pain-Group Treatment Facilitator and Patient ManualChronic pain management in manual therapy (OsteoMAP)
Chronic pain management in manual therapy (OsteoMAP)Guidelines for a flexibly structured, six session course for individual clients with persistent musculoskeletal pain, designed to be used by physical and manual therapists with brief ACT training. Resources include an explanatory covering letter, practitioner guide, practitioner and patient workbooks, and a preliminary research evaluation article.
(See also Abbey, H.A. (2017) Developing an integrated osteopathy and acceptance-informed pain management course for patients with persistent pain. (Doctoral Dissertation). University of Bedfordshire, UK.)
Communication Skills and ACT
Communication Skills and ACTPracticing communication skills can promote psychological flexibility and vice-versa. Teaching skill sets like Clean Talk and NVC may compliment ACT work.
Charlie Laurel, MS, LCMHC
Developmentally Disabled and Psychotic Individuals
Developmentally Disabled and Psychotic IndividualsAuthors note:
The co-morbidity of psychosis in individuals with developmental disabilities may exacerbate the financial strain, emotional turmoil, and difficulties in adaptive functioning that these individuals experience. Given the salience of distress across domains of functioning, there exists a pressing need for more effective interventions to address this population. I am posting this protocol in the hope that it will assist treatment practitioners working with the developmentally disabled. It is an attempt to create more "physicalized" ACT metaphors for clients who think more concretely. Please understand that ACT work with this population is evolving and that this protocol is a work in progress. An small single case study using this protocol was discussed in Pankey and Hayes, 2003.
Diabetes Management
Diabetes ManagementThe ACT for diabetes management protocol is available in book form in [[http://www.contextualscience.org/gregg_callaghan_hayes_2007|Gregg, J., Callaghan, G., & Hayes, S. C. (2007).]] The diabetes lifestyle book: Facing your fears and making changes for a long and healthy life. Oakland, CA: New Harbinger. Experimental tests to date: The ACT for diabetes management protocol is available in book form in Gregg, J., Callaghan, G., & Hayes, S. C. (2007). The diabetes lifestyle book: Facing your fears and making changes for a long and healthy life. Oakland, CA: New Harbinger. Experimental tests to date: Gregg, J. A., Callaghan, G. M., Hayes, S. C., & Glenn-Lawson, J. L. (2007). Improving diabetes self-management through acceptance, mindfulness, and values: A randomized controlled trial. Journal of Consulting and Clinical Psychology, 75(2) , 336–343.
Earliest ACT Protocols (aka "Comprehensive Distancing")
Earliest ACT Protocols (aka "Comprehensive Distancing")This page contains where are arguable the first two ACT protocols written while Dr. Hayes was at the University of North Carolina - Greensboro in 1981, and the earliest program written after Hayes moved to the University of Nevada, Reno in 1986 ... a protocol in 1987 by Sue Melancon (now Sue Melancon McCurry) for her predoctoral project with agoraphobia, submitted to the clinical psychology program at UNR in November 1988. All were described at the time as "Comprehensive Distancing" protocols but a detailed review finds references to the major components of nominally "ACT" protocols.
The first protocol is an unpublished five-page manual and is referred in Robert Zettle's 1984 dissertation as "Hayes, 1981". It is called "The Big D" after the lab's slang name for "comprehensive distancing."
The second is a manual for a study on comprehensive distancing for pain tolerance conducted in 1981/1982 and presented in this paper:
Hayes, S. C., Korn, Z., Zettle, R. D., Rosenfarb, I., & Cooper, L. (November 1982). Rule‑governed behavior and cognitive behavior therapy: The effects of comprehensive cognitive distancing on pain tolerance. Paper presented at the meeting of the Association for Advancement of Behavior Therapy, Los Angeles.
That study appeared in print in 17 years laer:
Hayes, S. C., Bissett, R., Korn, Z., Zettle, R. D., Rosenfarb, I., Cooper, L., & Grundt, A. (1999). The impact of acceptance versus control rationales on pain tolerance. The Psychological Record, 49, 33-47.
The pain tolerance protocol itself was long presumed to be lost but was discovered by Dr. Zettle in a cardboard box in his attic in 2024, misfiled with other papers. It is an onion skin carbon copy of a typewritten document, almost unreadable in physical form due to age, but easily readable as a scanned document with high contrast settings
The third is Dr. McCurry's pre-doctoral project (Melancon, 1988). It was based on a joint therapy client seen by Dr. Hayes and Sue Melancon as a graduate student in 1986-87, the transcripts of which formed the basis for the first protocols called "ACT." It is worth noticing that most of the modern elements of ACT including values are clearly in this Comprehensive Distancing protocol.
Enhancing supervisory relationships with values and committed action
Enhancing supervisory relationships with values and committed action ahessEpilepsy
EpilepsyAttached is the dissertation by Lundgren (2004) that includes the ACT for epilepsy treatment protocol.
Experimental tests to date:
Lundgren, T. (2004). Psychological treatment of epilepsy. Unpublished dissertation, Uppsala University, Uppsala, Sweden.
Lundgren, T., Dahl, J., Melin, L., & Kies, B. (2006). Evaluation of Acceptance and Commitment Therapy for drug refractory epilepsy: A randomized controlled trial in South Africa. Epilepsia, 47, 2173-2179.
Lundgren, T., Dahl, J., & Hayes, S. C. (2008). Evaluation of mediators of change in the treatment of epilepsy with Acceptance and Commitment Therapy. Journal of Behavior Medicine, 31(3), 225-235.
Experiential Adolescent Group Program
Experiential Adolescent Group ProgramLouise Hayes and Julie Rowse. (2008). Acceptance and Commitment Therapy: Experiential Adolescent Group Program. Also available from louiseh@unimelb.edu.au
The program is an 8 week group program for adolescents. The aim of the program is to use experiential mediums, for example painting or clay, to facilitate teenagers’ experience of the ACT concepts. Art allows them to explore their own experiences, without getting caught up in language processes.
The group program also makes use of role play and other forms of experience. Initial outcome data is positive and will be available from the first author early 2009. Artwork is shown in this document for training purposes only and should not be reproduced in anyway. All participant artwork has been used with written consent from the participants.
The program is designed for experienced ACT therapists to be modified as needed. It is not a step by step guide to ACT with young people. It is designed to be used flexibly, modifiying the content to fit with the particpants.
General Therapy Manual
General Therapy ManualNote: The manual attached below follows guidelines for the implementation of ACT derived from Acceptance and Commitment Therapy: An Experiential Approach to Behavior Change (1999) by Hayes, Strosahl, and Wilson.
As such, it is meant to supplement rather than serve as a replacement for this book in the implementation of ACT.
Accordingly, users of this manual should be familiar with the principles of ACT outlined in this book as well as additional techniques and procedures covered within it that are not explicitly contained in this manual.
(Thanks for this manual Rob Zettle!)
Handouts for General ACT Manual
Handouts for General ACT ManualHere are some handouts for homework assignments and in-session exercises.
Group Treatment of Depression
Group Treatment of DepressionExperimental tests to date:
Zettle, R. D., & Hayes, S. C. (1986). Dysfunctional control by client verbal behavior: The context of reason giving. The Analysis of Verbal Behavior, 4, 30-38.
Zettle, R. D., & Hayes, S. C. (1987). A component and process analysis of cognitive therapy. Psychological Reports, 61, 939-953.
Zettle, R. D., & Raines, J. C. (1989). Group cognitive and contextual therapies in treatment of depression. Journal of Clinical Psychology, 45, 438-445.
For further information contact: Robert Zettle (robert.zettle@wichita.edu), Wichita State University, Department of Psychology, 1845 N. Fairmount, Wichita, KS 67260-0034
H.E.A.T. (Honorably Experiencing Anger and Threat) Protocol
H.E.A.T. (Honorably Experiencing Anger and Threat) ProtocolSelect this link to access the HEAT (Honorably Experiencing Anger and Threat) group treatment protocol developed by Andy Santanello and Sharon Kelly.
Helping Psychotic Patients Cope with Positive Psychotic Symptoms
Helping Psychotic Patients Cope with Positive Psychotic SymptomsBach, P., & Hayes, S. C. (2002). The use of Acceptance and Commitment Therapy to prevent the rehospitalization of psychotic patients: A randomized controlled trial. Journal of Consulting and Clinical Psychology, 70(5), 1129-1139.
Heroes and Addiction
Heroes and AddictionLessons using the "hero" to create a life beyond addiction. This curriculum includes 3 lessons focusing on 1. Heroes 2. Values 3. Your Cause
Injured Talk vs Courageous Talk_Heroes and Communication
Injured Talk vs Courageous Talk_Heroes and Communication smswabyLiving By Committed ACTion Workbook
Living By Committed ACTion WorkbookThe following six-module workbook was created by a group of psychologists working in Nova Scotia, Canada.
Although initially created as a workbook to be used in group settings, it was adjusted so that it could also be used as a guided self-help intervention. During the Covid-19 pandemic, this workbook has been provided to clients for self-directed reading and practice (using the guided exercises hyperlinked in the document). Clients were also offered brief telephone coaching appointments during the six week program.
Clinical response and client satisfaction have been tracked and in-house program evaluation has revealed positive outcomes.
Contact: sjbaileyphd@gmail.com
Living Well Beyond Pain and Illness
Living Well Beyond Pain and IllnessA 3 manual protocol for a 6 week group or individual treatment using ACT and Mindfulness for managing chronic pain and/or chronic illness. Consists of client booklet, facilitator manual and Mindful movement and exercise program. Can be used in health care settings and in private practice.
Questions or queries to Dr C A Phillips christinea54.phillips@gmail.com
Math Anxiety
Math AnxietyBelow is the ACT for math anxiety protocol developed by Zettle (2003).
Experimental tests to date:
Mindfulness and Acceptance-based Group Therapy for Social Anxiety Disorder
Mindfulness and Acceptance-based Group Therapy for Social Anxiety DisorderMindfulness and Acceptance-Based Group Therapy for Social Anxiety Disorder: A Treatment Manual, Second Edition
Mindfulness and Acceptance-Based Group Therapy for Social Anxiety Disorder: A Treatment Manual, Second EditionThe second edition of Mindfulness and Acceptance-Based Group Therapy for Social Anxiety Disorder: A Treatment Manual is a revision of the treatment protocol used in the following two studies:
We revised the manual in order to incorporate new terminology and exercises from our self-help book, The Mindfulness and Acceptance Workbook for Social Anxiety and Shyness, published by New Harbinger in 2013. For example, we introduced the acronym VITAL as a handy way to remember to: V- base actions on your Values and goals; I - remain In the present moment; T- Take notice of your feelings, thoughts, and urges (from your observer perspective); and AL -Allow your experience to be exactly as it is. Accordingly, the term used for willingness/exposure exercises is Taking VITAL Action.
We have been using the revised manual with our therapy groups since September 2013 and have received positive feedback from clients. Therapists have found it to be more “user friendly” than the original protocol.
The second edition of the treatment manual includes a detailed therapist manual, all client handouts, and is used in conjunction with The Mindfulness and Acceptance Workbook for Social Anxiety and Shyness and the downloadable mindfulness exercises which accompany that book.
Mindfulness and Acceptance-based Group Therapy for Social Anxiety Disorder: A Treatment Manual
Mindfulness and Acceptance-based Group Therapy for Social Anxiety Disorder: A Treatment ManualThe manual is also available on request from the authors in a Word document.
If you use the manual please let us know - we are tracking its use. We also welcome any type of feedback.
Mindtrain- ACT treatment manual for therapists working with anxious children
Mindtrain- ACT treatment manual for therapists working with anxious childrenMindtrain treatment manual together with ausio recordings for child-friendly mindfulness meditations, can be accessed from the following link:
https://www.dropbox.com/sh/20ffnay3pt2kh5u/AADlHF8Pl2sMuTHORZxH7f0Xa?dl=0
OCD
OCDAn eight session ACT for OCD protocol.
Twohig, M.P., Hayes, S.C., Plumb, J.C., Pruitt, L.D., Collins, A.B., Hazlett-Stevens, H., & Woidneck, M.R. (2010). A randomized clinical trial of acceptance and commitment therapy vs progressive relaxation training in the treatment of obsessive compulsive disorder. Journal of Consulting and Clinical Psychology, 78, 705-716.
Twohig, M. P., Hayes, S. C., & Masuda, A. (2006). Increasing willingness to experience obsessions: Acceptance and Commitment Therapy as a treatment for obsessive compulsive disorder. Behavior Therapy, 37(1), 3-13.
For further information contact: Mike Twohig (michael.twohig@usu.edu), Assistant Professor, Utah State University, Department of Psychology, 2810 Old Main Hill, Logan, Utah 84322-2810, www.twohig.usu.edu.
ACT for OCD: Abbreviated Treatment Manual translated to Arabic
ACT for OCD: Abbreviated Treatment Manual translated to Arabicعلاج التقبل و الإلتزام لإضطراب الوسواس القهري: كتيب العلاج المختَصر (ACT for OCD: Abbreviated Treatment Manual un-validated translation by Tamer Sedky Zeidan)
ترجمه: تامر محمد صدقي زيدان طالب دكتوراه في الطب النفسي كلية الطب، جامعة عين شمس 2019
Communication au symposium Pleine Conscience des 37èmes Journées Scientifiques de l'AFTCC, Paris 12 décembre 2009
Communication au symposium Pleine Conscience des 37èmes Journées Scientifiques de l'AFTCC, Paris 12 décembre 2009Étude pilote de prise en charge en groupe par l’ACT de patients TOC rechutés et/ou résistants et souffrant de comorbidité et suivi à 1 an. B. SCHOENDORFF (1), B. PUTOIS (2), C. BARNEL (3), E. MOLLARD (4) (1) Université Claude Bernard, Lyon (2) Université Louis Lumière, Lyon (3) Hôpital cardiologique Louis Pradel, Lyon (4) Hôpital neurologique Pierre Wertheimer, Lyon Communicant : Benjamin PUTOIS bputois@gmail.com
Problématique : En proportion non négligeable, des patients souffrant de TOC ne répondent pas aux meilleurs traitements validés (TCC et/ou ISRS). Cette population souffre souvent de comorbidités tels des troubles de la personnalité. Cette étude pilote évalue l’efficacité potentielle d’un traitement ACT en groupe chez cette population.
Méthode : Étude pilote sous forme de groupe fermé (11 séances d’intervention manuélisées et 3 séances de suivi) à l’hôpital Wertheimer de Lyon, N=9. 6 participants présentaient une comorbidité, dont 5 troubles de la personnalité. YBOCS moyen 28,7. 11 groupes hebdomadaires de 3 heures pendant 11 semaines puis suivi à 3 mois, 6 mois et 1 an. Mesures principales : Y-BOCS, et mesures autoévaluées de handicap, temps passé et malaise dû aux obsessions/compulsions. Nombreuses autres mesures dont AAQ (Hayes), MAAS (Brown&Ryan) et de qualité de vie (Marks).
Résultats : Les 9 participants ont complété l’étude, mais seulement 7 ont participé aux séances de suivi. L’acceptabilité du traitement était bonne chez tous les participants, et haute à très haute chez 6. L’amélioration pré-post du score Y-BOCS était significative pour le groupe de 9 (z=2,67, p<,01 ; d=2,13) et maintenue à tous les points de suivi (3 mois, 6 mois et 1 an) pour les 7 participants présents aux séances de suivi (suivi 1an : z=2,34 ; p=,02 ; d=1,92). L’effet du traitement était également significatif sur la dimension handicap (à 1 an : p<,05 ; d = 0,91), et tendanciel sur la dimension malaise (à 1 an : p= 07 ; d=0,99).
Discussion : Cette étude pilote de type « preuve de concept » suggère que l’ACT peut présenter une intervention adaptée et acceptable chez les patients « difficiles » souffrant de TOC résistants et/ou rechutés et souffrant d’importantes comorbidités. On peut faire l’hypothèse que les interventions de défusion cognitive, visant à distancer radicalement des pensées sont particulièrement bien adaptées à un trouble dont les victimes souffrent au premier chef de la tyrannie de pensées qui se « collent à eux » et contre lesquelles ils combattent en vain. On remarquera aussi la forte acceptabilité du traitement chez cette population réputée difficile.
Pole to Pole: An approach for exploration and communication in bipolar
Pole to Pole: An approach for exploration and communication in bipolarLaura Walton, Gordon Mitchell, Lindsay-Jo Sevier-Guy, Stephanie Fagan, Emma Butchard, Graeme Babbs and members of Fife Bipolar Group
The Psychological Interventions for Psychosis (PIP) Service, within NHS Fife Clinical Psychology Department, provides psychological approaches for psychiatric conditions including psychosis and bipolar disorder. The service has links with various non-statutory and voluntary agencies supporting people affected by these conditions, and one such link is with the Fife Bipolar Group; a local branch of Bipolar Scotland. Over the last few years, our two organisations have been collaborating in the development of a new resource for people affected by bipolar disorder. The resource has been designed for people with a diagnosis of bipolar disorder; the people in their lives (i.e. family and friends); and professionals who work with people with bipolar disorder (e.g. healthcare workers).
The approached is based upon the principals of ACT and, through consultation with members of Fife Bipolar Group it evolved around the theme of travel, i.e. living with Bipolar being a journey. This is how it came to be called Pole to Pole. The name Pole to Pole simultaneously recognises the bipolar nature of emotional experience and the concept of exploring this experience. The approach consists of a resource pack, containing activities to explore experiences and values, which people are guided through in three group sessions. The sessions are designed to help people to reflect openly on their experiences of bipolar, whether directly or as a carer, and to communicate about the impact the condition has had in their lives. The activities are to create a Map of emotion experiences, a Guide based on values, a Compass to direct value-living and a Travelog to record and reflect upon experience. We also include additional experiential exercises in the sessions to deliver concepts such as acceptance and valued-living.
The purposes of Pole to Pole are to assist people with bipolar disorder and their carers to: learn more about mental, physical and emotional states; identify values and obstacles that get in the way of valued living; develop ways to work around the obstacles; and communicate with others about emotional experiences and values. Pole-to-pole may also be used to communicate with healthcare professionals about experiences of bipolar.
Our manual, pdfs of session Powerpoint presentations and pdfs of the activities are attached here.
Postpartum Depression
Postpartum DepressionAn ACT protocol designed for use with postpartum depression. For further information contact: Espen Klausen
Psilocybin-Assisted Therapy of Depression using ACT (Yale Manual)
Psilocybin-Assisted Therapy of Depression using ACT (Yale Manual)The Yale Manual for Psilocybin-Assisted Therapy of Depression provides researchers and therapists with methods, structure, and areas to consider regarding the use of psychedelic- assisted therapy in the treatment of Major Depressive Disorder (MDD). In particular, this manual illustrates a mode of utilizing Acceptance and Commitment Therapy (ACT) as a therapeutic framework for psilocybin-assisted therapy of depression.
For information, write to Dr. Jordan Sloshower: Jordan.Sloshower@yale.edu
Psychotherapy for methamphetamine dependence
Psychotherapy for methamphetamine dependenceScubaFlex: ACT for Scuba Divers
ScubaFlex: ACT for Scuba DiversThe "ScubaFlex: ACT for Scuba Divers" protocol brings Acceptance and Commitment Therapy (ACT) with scuba diving. Crafted by Laura and a few stranded scuba divers in response to pandemic-era challenges, the guide provides a comprehensive introduction to all ACT processes through the lens of scuba diving, with a focus on achieving psychological flexibility. Each session of the program, enriched by participant feedback and insights, explores a unique aspect of ACT, embodying a playful reinvention of the hexaflex. The protocol delivers a structured yet adaptable approach, encouraging ACT practitioners to infuse their expertise into the program and align it with their participants' needs. From values and mindfulness to defusion and committed action, every topic is addressed in the context of the diving experience.
We are deeply grateful to the ScubaFlex participants for their involvement and to the wider ACT community for their original exercises and practices. This manual is not just a resource, but an invitation to dive deeper into self-understanding and psychological flexibility, above and below the water's surface. Our heartfelt thanks to all who have joined us on this journey.
If you are interested in participating in a group, details are available on fittodive.org. If you would like to run the group yourself, and have appropriate qualifications and experience, the protocol is freely available. If you would like to carry out research of it's effectiveness, please get in touch!
Self-Help Manual for Anxiety and/or Depression
Self-Help Manual for Anxiety and/or DepressionDear ACT community,
We would like to share with you a brief manual which is being developed as part of Doctorate in Clinical Psychology to help those with anxiety and/or depression.
The manual is designed to be accompanied with two therapist telephone calls to guide clients through the manual. It is a brief 58-page document that has been specifically designed to be photocopied in grey scale with ease. We are currently conducting a randomised controlled trial to invesigate the effectiveness of guided self-help, compared to a non-active control condition using this manual. Some pages are specific to a Scottish audience for this reason but please contact us if you feel it could be of some use and we can then adapt it.
The manual contains a chapter on each of the six ACT processes (present moment awareness, cognitive defusion, acceptance, self-as-context, connecting with values and committed action). It is designed so that one chapter is read each week (6 weeks in total) with behavioural tasks at the end of each chapter. It has been deemed 'fairly easy to read', with a Flesh Reading Ease Score of 69.6.
We will seek to post the results of the first study on the ACBS website as soon as they are ready.
Best wishes,
Shane Ford (shanealwynford@hotmail.com)
Co-authors: Dr David Gillanders (david.gillanders@ac.ed.uk)
Self-Stigma and Shame in Substance Addiction
Self-Stigma and Shame in Substance AddictionThe treatment manual attached below was originally developed through an iterative process as described in:
The intervention was then tested in a randomized clinical trial, the results of which are published here:
Abstract
Objective: Shame has long been seen as relevant to substance use disorders, but interventions have not been tested in randomized trials. This study examined a group-based intervention for shame based on the principles of Acceptance and Commitment Therapy (ACT) in patients (N = 133; 61% female; M = 34 years old; 86% Caucasian) in a 28-day residential addictions treatment program. Method: Consecutive cohort pairs were assigned in a pair-wise random fashion to receive treatment as usual (TAU) or the ACT intervention in place of six hours of treatment that would have occurred at that same time. The ACT intervention consisted of three, two-hour group sessions scheduled during a single week. Results: Intent-to-treat analyses demonstrated that the ACT intervention resulted in smaller immediate gains in shame, but larger reductions at four month follow up. Those attending the ACT group also evidenced fewer days of substance use and higher treatment attendance at follow up. Effects of the ACT intervention on treatment utilization at follow up were statistically mediated by post treatment levels of shame, in that those evidencing higher levels of shame at post treatment were more likely to be attending treatment at follow up. Intervention effects on substance use at follow up were mediated by treatment utilization at follow up, suggesting that the intervention may have had its effects, at least in part, through improving treatment attendance. Conclusions: These results demonstrate that an approach to shame based on mindfulness and acceptance appears to produce better treatment attendance and reduced substance use.
You can get both of the articles here.
The fidelity coding system used in the JCCP article is also below. Please contact Jason Luoma for consultation if you choose to use this treatment manual to replicate these findings or need help with the fidelity coding system. We'd also appreciate any input from people who choose to use this protocol in research or in treatment settings. Let us know how it goes or provide feedback to improve it.
As part of a newer study in Russia, our team created a revised version of the manual and then translated it to Russian. The newer manual is more detailed and more structured than the original and probably easier to use for most clinicians. This manual is currently being tested and results will be listed here when we know the results. In the meantime, the English version of the newer manual is also attached below (you need to be logged into see it) and free to use for research and clinical purposes. We also developed an updated fidelity coding system that is available upon request.
If you are interested in helping with the research on self-stigma, consider contacting the Self-Stigma Research Collaborative.
Severe Substance Abuse Problems
Severe Substance Abuse ProblemsThe attachments contain the individual and group ACT protocols (and group handouts) that were designed for use in severe substance abuse problems and were tested in:
An Individual ACT protocol designed for use in severe substance abuse problems. Experimental tests to date: Hayes, S. C., Wilson, K. G., Gifford, E. V., Bissett, R., Piasecki, M., Batten, S. V., Byrd, M., & Gregg, J. (2004). A randomized controlled trial of twelve-step facilitation and acceptance and commitment therapy with polysubstance abusing methadone maintained opiate addicts. Behavior Therapy, 35, 667-688.
Note that the group manual was set up to support the individual manual ... it is not designed for use by itself. Exp
If you have questions email the researchers ... don't just post a comment here (there is not procedure that forwards that to the researchers and there are thousands of pages on this website)
Skin picking
Skin pickingThe treatment protocol for the ACT for skin picking study is exactly the same as the one for the OCD study by the same authors. All you need to do is change the word "obsession" to "urge to pick" and it will fit nicely.
Twohig, M. P., Hayes, S. C., & Masuda, A. (2006). A preliminary investigation of ACT for chronic skin picking. Behaviour Research and Therapy, 44, 1513-1522.
Stigma Toward People With Psychological Disorders
Stigma Toward People With Psychological DisordersBelow is a protocol for a two and a half hour workshop on ACT for stigma toward people with psychological disorders developed by Akihiko Masuda, Kara Bunting and Steven Hayes. The psychoeducation control protocol used in Masuda et al. (2007) is also included.
Experimental tests to date:
Masuda, A., Hayes, S. C., Fletcher, L. B., Seignourel, P. J., Bunting, K., Herbst, S. A., Twohig, M. P., & Lillis, J. (2007). The impact of Acceptance and Commitment Therapy versus education on stigma toward people with psychological disorders. Behaviour Research and Therapy, 45(11), 2764-2772.
The ACT Matrix
The ACT MatrixKevin Polk is in private practice and at the VA in Togus, Maine, USA has collaborated with Jerold Hambright and Mark Webster to develop "The Matrix" as a way of thinking about and engendering psychological flexibility. It is a simple yet elegant way to understand and experience the complex phenomenon of being human.
[Kevin runs ongoing "The ACT Matrix" webinars and consultations each month. Go to www.theactmatrixacademy.com to sign up.]
The Matrix is a simple to use format developed initially for groups, but then came into wide use with individuals. Based on an original idea by Kevin Polk the format was co-developed with Mark Webster and Jerold Hambright. It is based on learning to discriminate between direct experiencing with the senses and indirect experiencing in the mind (vertical line), and then the idea of sorting behavior into two directions called Towards and Away (horizontal line). The two lines of the matrix intersect in the middle at 90 degree angles. The four quadrants created by the two lines contain the following four categories that are asked in the following order:
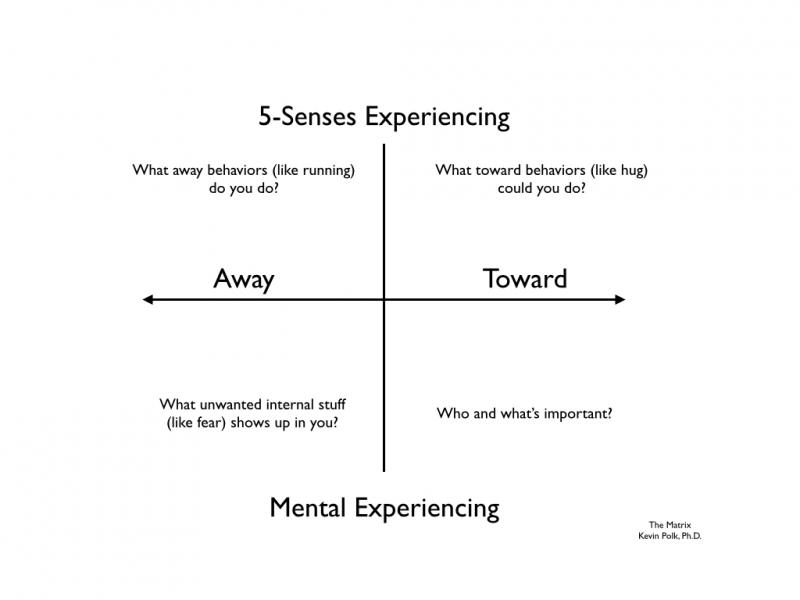
Learning to use the Matrix is experiential and much the same as learning to ride a horse, or a bike, or play the piano, or paddle a kayak. It is a simple idea that can be learned very quickly but takes a little time and practice to become proficient. Mainly people practice learning to notice where behaviors are taking them, and to align that with what is important. The simplicity of the model means that it is broadly applicable and can be used outside of the clinical setting, for instance it is already used in education and in the workplace. It's been used in Sierra Leone to help combat the spread of the Ebola virus and in prisons to help inmates improve value consistent behaviors.
Read more about Polk's work on his Psychological Flexibility Blog.
Check out the free ACT Matrix Course here...
Mark Webster has also created a 3 part video series introducing the ACT Matrix which can be found here:
To Learn more also see Kevin Polk's training page as well as his Website.
Click here for upcoming workshops and trainings.
Below you will find various handouts and .pdfs about the matrix cultivated from trainings anf conference presentations.
Charlie Laurel ACT Videos
Charlie Laurel ACT VideosI created these four videos on the ACT matrix to help my professional colleagues use the matrix with compassion and flexibility. The first video goes through the basic description; the second presents a made-up case to illustrate use; the third presents some of the insights that can emerge from matrix work; the fourth is an experiement with a double matrix to illuminate the complexity of moving toward change when two people are interacting, and possibilites to break unworkable cycles of behavior. I hope you find them useful.
Charlie Laurel, MS, LCMHC
Kevin Polk Page
Kevin Polk PageAn Introduction to ACT- for Rapid Behavior Change

The Matrix represents the two primary mechanism of change in ACT that are called Perspective Taking and Behavioral Analysis. Unlike typical behavioral analysis in which a practioner does the analysis, in ACT we teach the client to do her or his own analysis. In it's simplest form, the person learns to notice behaviors that move Toward values or Away from unwanted experiencing. Both Toward and Away moves are essential to life, it's the combination of the moves over time that add up to living a relatively stuck life, or one that is moving toward values. Said another way, it's a way of noticing a combination of behaviors that work for living a valued life.
You can use the Matrix a million different ways. Below is a video course about Psychology Flexibility Training that can be presented to community groups.
I offer online and telephone training to professionals doing mental health or process improvement work.
You can contact me or visit the website at www.drkevinpolk.com for more information.
A great way to get started with the Matrix is the Visual Wellness Plan.
You can get the "Visual Wellness Plan" manual by clicking here.
Be well,
Kevin
Learning the Matrix
Learning the MatrixThe Matrix is a simple method for teaching clients to understand the function of their behaviors (e.g., avoidance/escape versus moving toward values) as well as discriminate between events within and outside the skin (e.g., mental experiencing and direct experience). It was created by Kevin Polk, Mark Webster, and Jerold Hambright.
Here are links to three videos (on Youtube) that details the Matrix and demonstrates how to use it.

http://www.youtube.com/watch?

http://www.youtube.com/watch?

http://www.youtube.com/watch?
Attached to this page is a companion document that walks you through using it with clients.
The MATRIX Worksheet w/ Fill in Blanks and Excel Codes
The MATRIX Worksheet w/ Fill in Blanks and Excel Codes pmcnulty1000The Matrix in Swedish
The Matrix in SwedishACT-matrisen är ett sätt att ge ACT. För att läsa mer om ACT-matrisen rekommenderas “The ACT Matrix” och “The Essential Guide to the ACT Matrix”. Den senare boken har fått stå som förlaga till denna svenska anpassning. Thor Bengtsson är alltså inte upphovsman till The ACT Matrix men har stått för denna översättning och anpassning till svenska. Det kan vara svårt att förstå denna svenska bearbetning helt och hållet om man inte läst åtminstone den senare boken. Utöver ovanstående läsrekommendationer är det viktigt att behärska ACT i allmänhet och även vara förtrogen med patient/klientgruppen. Handledning föreslås till den osäkre och även ibland för den säkre.
I sex steg ger vi deltagarna kraftfulla verktyg att själv kunna relatera till och hantera till sina problem. De sex stegen är som följer:
Presentation av matrisen, en sortering av beteenden i en fyrfältare med axlarna “Till och Från” och “Inre och Yttre”.
Funktionell analys av problembeteenden (Att jämföra med, ABC, T-K-H eller SORK)
Medvetandegörande av problembeteenden (Metafor: Att inte bita på krokar)
En modell med verbala hjälpmedel för att applicera svåra situationer på ACT-matrisen och inte fastna i problembeteenden (Metafor: Verbal Aikido)
Self-Compassion (här har det blivit störst förändringar mot förlagan)
Träning i perspektivtagande (Att ta perspektiv med sig själv vid andra tidpunkter)
Materialet finns nedan
Observera att uppdateringar sker löpande.
The Survival-Vital Matrix
The Survival-Vital MatrixA spin on the traditional ACT Matrix.
Attached is a quick-guide to the S-V Matrix, and more information can be found here: https://www.theactmatrix.com/pages/trauma
And here is a video elaborating on this version: https://youtu.be/hTJXPYRYI5s
The matrix in spanish
The matrix in spanishBelow is a version of the matrix in spanish. Enjoy! Fabián
The ACT Matrix for Intake Sessions
The ACT Matrix for Intake SessionsHere's how to use the ACT Matrix for the first time with a client, including scripts of how to phrase things.
It covers creative hopelessness, goal setting, therapeutic alliance and tips and tricks to setting up the ACT Matrix in a clear and comprehensive way.
The ACT Roadmap - A Free Guide for getting started with ACT
The ACT Roadmap - A Free Guide for getting started with ACTThe ACT Roadmap is a FREE 28 page Ebook for learning about Acceptance and Commitment Therapy (ACT).
With its colourful design, this digestible guide teaches you about ACT practice's head, hands, and heart. You'll learn about Contextual Behavioural Science (CBS), the home of ACT, receive guidance on treatment, supervision and relevant resources to build your knowledge and skills.
Written by Jim Lucas, ACBS Peer-reviewed ACT Trainer.
You can download a FREE copy here.
The ACT Roadmap is available in Portuguese: Roteiro ACT - Guia de Introdução à Terapia de Aceitação e Compromisso
Trichotillomania
TrichotillomaniaThe protocol is available in book form in
Woods, D. W., & Twohig, M. P. (2008). Trichotillomania: An ACT-enhanced Behavior Therapy Approach Therapist Guide. Oxford University Press.
The accompanying client workbook is available in
Woods, D. W., & Twohig, M. P. (2008). Trichotillomania: An ACT-enhanced Behavior Therapy Approach Workbook. Oxford University Press.
Experimental tests to date:
Woods, D. W., Wetterneck, C. T., & Flessner, C. A. (2006). A controlled evaluation of Acceptance and Commitment Therapy plus habit reversal for trichotillomania. Behaviour Research and Therapy, 44(5), 639-656.
Values List & Tool
Values List & ToolFrom Ellie Miller:
I've created a simple Values List PDF and an Interactive Online Tool to help your clients pinpoint what's truly important to them.
These easy-to-use resources are great for guiding clients through ACT values clarification, whether as part of homework or during live sessions via screen sharing.
They're practical, straightforward, and ready to be integrated into your work. Give them a try and see how they can support your clients' progress.
Check it out here → Values List & Interactive Tool
 (2 x 2.5 in).png)
100+ ACT Journal Prompts
100+ ACT Journal PromptsElevate your clients' reflective practice with our expansive collection of over 100 ACT-themed journal prompts. Designed to inspire deeper self-exploration and align with core ACT principles, this generator is an invaluable tool for therapists seeking to enrich their clients' homework and session work. It’s a perfect resource for sparking meaningful insights and facilitating personal growth, available at your fingertips.
→100+ ACT Journal Prompts for Self Reflection
Visual Aid for explaining how the Observing Self relates to our brain
Visual Aid for explaining how the Observing Self relates to our brainHi,
I have adapted some slides from Dr Janina Fisher- to explain how making contact with our Observing Self can help dampen the effects of our Amygdala on our FIght/flight responses. I hope that you find them useful. I would be most welcome to feedback.
Kind regards,
Campbell
Weight Maintenance
Weight MaintenanceExperimental tests:
Lillis, J., Hayes, S. C., Bunting, K., & Masuda, A. (2009). Teaching acceptance and mindfulness to improve the lives of the obese: A preliminary test of a theoretical model. Annals of Behavioral Medicine, 37, 58-69.
Below is a protocol for a 1-day workshop for weight-related stigma and weight maintenance based on Acceptance and Commitment Therapy developed by Jason Lillis, Steven Hayes, and Kara Bunting.
Worksite Stigma and Burnout
Worksite Stigma and BurnoutThis is a protocol designed to reduce entanglement with stigmatizing thoughts about clients and through that reduction in burnout and stress at work.
Experimental tests:
Hayes, S. C., Bissett, R., Roget, N., Padilla, M., Kohlenberg, B. S., Fisher, G., Masuda, A., Pistorello, J., Rye, A. K., Berry, K. & Niccolls, R. (2004). The impact of acceptance and commitment training and multicultural training on the stigmatizing attitudes and professional burnout of substance abuse counselors. Behavior Therapy, 35, 821-835.
The protcol is for a 6 hour group workshop. It is not very detailed -- refering in a single line to exercises that might take 40 minutes. For those familiar with experiential ACT workshops, this should be enough. You will see most of these exercises at major ACT / RFT conventions such as the World Conferences or the Summer Institutes.
This protocol is currently being revised for a large new grant (which will run from 2005 to 2008) that will replicate and extend the study above. It is our sense that we can do better than the protocol that is here, so don't feel bound by it. Use it as a starting point.
The adherence manual include both ACT and Multicultural Training items since that was the comparision in the study (and in this new grant ... which will include an ACT and MT combination group as well as ACT alone and MT alone and a control).
For more information contact Steve Hayes (hayes@unr.edu), Department of Psychology, University of Nevada, Reno, NV 89557-0062
Worksite Stress Interventions
Worksite Stress InterventionsExperimental tests to date:
Bond, F. W., & Bunce, D. (2000). Mediators of change in emotion-focused and problem-focused worksite stress management interventions. Journal of Occupational Health Psychology, 5, 156-163.
The protocol itself can be found in Bond, F., & Hayes, S. C. (2002). ACT at work. In F. Bond & W. Dryden (Eds.), Handbook of Brief Cognitive Behaviour Therapy (pp. 117-140). Chichester, England: Wiley.
For further information contact: Frank Bond (f.bond@gold.ac.uk), Department of Psychology, Goldsmiths College, University of London, New Cross, London SE14 6NW
Worksite stress interventions II: Brief ACT-enhanced MBI for hospital ward staff
Worksite stress interventions II: Brief ACT-enhanced MBI for hospital ward staffThis course was designed for frontline hospital staff who were unable to attend a standard 8-week course in working hours, because of workload/staffing pressures. The course was delivered as 8 half-hour sessions WITHIN the hospital ward, in a quiet room, whilst their colleagues willingly covering their duties. The approach is based on MBCT, ACT and a self compassion exercise (made by combining ACT metaphor with an exercise provided by Choden and Paul Gilbert).
1 page Summary course overview is given in poster format below
Materials for the 8-week course, are supplied, organised by week. (Plus Week 0, which was the taster session). Includes all course materials, scripts, teacher timetables (we needed detailed timings because each session was only half an hour long, and we kept to these timings so that clinical work was not affected); we've also included a few reflections on how sessions went and how we'd do it differently next time, and equipment checklists. Mp3s for raisin and chocolate meditations are provided, and the other audio tracks are available with the course handbook (Peace in a Frantic World, Mark Williams and Danny Penman).
Measures: Another time, we would probably use different pre and post measures (these were selected based on local factors), e.g. GHQ12; the written qualitative questions yielded a lot of useful information; also staff were keen to express their thoughts in a facilitated meeting with the Senior HR manager Antony who championed the pilot.
Please feel free to use and adapt
Margo Campbell (ACBS member), Richard Hawkins, Antony Cobley (not ACBS members)
Young Children
Young ChildrenExperimental tests to date: None Published For further information contact: Amy Murrell (amurrell@unt.edu) or Kelly Wilson (kwilson@olemiss.edu), University of Mississippi. Author's note: We are posting this protocol in the hope that they will provide useful information in helping clients and spark further interest and research in ACT with children and adolescents. Please, recognize that we consider the treatment technology to be evolving in nature. These protocols, therefore, should be viewed as works in progress. The underlying principles should be adhered to, but the protocols can (and indeed should) be used with flexibility.
Organizing Sessions
Organizing SessionsACT Session Checklist
ACT Session ChecklistWhat is it?
The attached Word files are intended for ACT Clinicians to monitor their fidelity to the treatment principles of ACT. This is done by rating the therapist's practice immediately after each session.
Essentially the "ACT Core Competency Session Rating Form" is a less wordy form of the Core Competencies self rating form. The difference is that this form I've uploaded has very brief, generally three-word, descriptions of the items from the Core Competencies Self Rating Form. If you want to see how each item in the "Session Rating Form" corresponds to the ones in the "Competencies self rating form", read the "ACT Core Therapeutic Session Checklist Cross reference" file below. The Session rating form also has a checkbox for each session so that the sheet can be used for ten sessions with the one client.
How does it work?
You can score it in a number of ways. Here are some examples:
- Check mark or cross in the box for presence of the dimension/behavior;
- Check mark or cross for absence of the dimension/behavior;
- Combination of both of the above - check for presence, cross for absence, dash for neutral or not applicable;
- Score from say, 0 to 10 for degree/quality/frequency of the dimension/behavior.
Obviously if you're using this for research or for practitioner training, evaluation or supervision, you need a consistent approach across sessions and clients. N.B. US version is for Letter sized paper, UK version for A4.
Why did you do it?
I haven't had the opportunities that many ACT practitioners have had of being immersed in an ACT-focused research program or of attending a Summer Institute or World Conference. Consequently I've been trying to improve my ACT practice without the benefit of observational 'live' supervision. I've used this kind of self-monitoring sheet when learning other therapeutic approaches and found it very helpful. Using this kind of self-monitoring session rating sheet is one way I believe, of achieving expertise through effortful practice.
What's next?
If you download the session rating form and use it, please post your opinions, comments, suggestions for change/revision and findings here. If you have an extended comment or heaven forbid, actually use it in research or formal practitioner training, I'd suggest making a child page here.
As well, I'd ultimately like to see the 60-odd items here reduced to a manageable 12 or less. Workability of the tool will ensure its use. Parsimony, validity and reliability are essential.
The attached spreadsheet gives some idea of the direction in which I think this endeavour could develop. I've proposed six 'global dimensions' of in-session therapist behavior. They are Structure, Flexibility, Workability, Presence, Precision and Compassion.
These dimensions are not the same as the dimensions of the Hexaflex because the Hexaflex describes processes and I am attempting to describe either therapist traits or if you like, 'therapist qualities demonstrated in session'. Clearly though there is some degree of overlap - Being Present with Presence, and Acceptance with Flexibility (but also with Compassion).
I've developed these 'global dimensions' to give the therapist some 'touchstones' or compass points for their own practice. I welcome practitioners', trainers' and researchers' comments on any of these documents.
Business Card Behavioral Analysis
Business Card Behavioral AnalysisI've been using a process with both group, couple, and individual clients that seems to work pretty well. I stumbled upon this, but I'm sure it's been thought of before. If someone has refinements, I'd love to hear it.
I've been using the back of old business cards to conduct a chain analysis of behaviors with clients. Business cards seem to be just the right size for this, as you can't really put much on them. I have the clients write down all of the pieces of the situation, behavioral chain, what have you, and then they lay them out.
The cool thing is, sometimes they'll lay out two cards that seem to have a lot more to them, and I can challenge them to make sure there's no more steps. For example, my mother calls me on one card, I want to die, on the next. We can tease apart all of the behavioral steps in the chain, group different parts together, shift them around, add new or different steps, change the order. It seems to work pretty well for defusion and self as context.
At the end of the session, clients take their business card chains home with them, and bring them back to session the next time. We talk about walking even with the cards in their pockets.
It's fun.
Core Processes/Metaphors Tracking
Core Processes/Metaphors TrackingCore Processes/Metaphors Tracking
Have you ever had this situation: You are meeting with your sixth patient of the day and, in the therapeutic moment, you see a perfect opportunity to present a particular ACT metaphor....but you can't quite remember if you had done that other metaphor which sets the stage for this one.....and you ask "have we talked about the person in the hole yet?" Now, many of the perfect therapists on this list surely would never do this. However, for the rest of us, how do you keep track of what you have covered?
I designed the attached form (see bottom) for jotting down what I have covered. I sometimes review it prior to sessions along with progress notes from those earlier sessions. Now, granted, I still occasionally check-in about whether we covered an exercise/metaphor (no big deal), though less often and less awkwardly. You will note that the exercises and metaphors often target multiple core processes, so this form is just a coarse tracking guide. But I find it helpful.
Content of the Attachment
Page 1 is the form. Page 2 is an example of what it might look like after multiple sessions (metaphors/exercises would be hand-written, of course). Upon review, the sample on Page 2 contains far more actual content than the completed forms I have used with patients.
Using the Form
Time proceeds from middle (1st session) to out (in my use of it). Going from out to in results in much crowding of the content in the middle. It also makes it more difficult to get a sense for the progress of therapy (at a glance).
Using the Form for Self-Assessment
The form can also be used as a tool for ongoing self-assessment, revealing your therapy habits. For example, even a casual glance at some of my completed forms quickly revealed that I favor Values work and Cognitive Defusion, using a handful of mindfulness techniques, mostly for getting clients and myself into the Present Moment, less so in the service of promoting Self-As-Context. While this evident pattern may merely reflect my personal style in using ACT, it also challenges me to do some self-examination about processes that I may avoid (one's style is always a work in progress, right?). I also find it useful to compare completed forms to my responses on the ACT Core Competency Self-Assessment, an excellent learning tool available on this site.
Improvements and Revisions
Feel free to edit, change, and improve the Core Processes/Metaphors Tracking Form to fit your needs. If others have similar tools/guides or improve upon this form, please share the work!
Techniques and Components
Techniques and ComponentsFacing the Current Situation ("Creative Hopelessness")/Control is a Problem
Facing the Current Situation ("Creative Hopelessness")/Control is a ProblemPurpose: To notice that there is a change agenda in place and notice the basic unworkability of that system; to name the system as inappropriately applied control strategies; to examine why this does not work
Method: Draw out what things the client has tried to make things better, examine whether or not they have truly worked in the client’s experience, and create space for something new to happen.
When to use: As a precursor to the rest of the work in order for new responses to emerge, especially when the client is really struggling. You can skip this step in some cases, however.
Things to avoid: Never try to convince the client: their experience is the absolute arbiter. The goal is not a feeling state, it is what the Zen tradition calls “being cornered.”
Examples of techniques designed to increase creative hopelessness:
| Creative hopelessness | Are they willing to consider that there might be another way, but it requires not knowing? |
| What brought you into treatment? | Bring into sessions sense of being stuck, life being off track, etc. |
| Person in the Hole exercise | Illustrate that they are doing something and it is not working |
| Chinese handcuffs Metaphor | No matter how hard they pull to get out of them, pushing in is what it takes |
| Noticing the struggle | Tug of war with a monster; the goal is to drop the rope, not win the war |
| Driving with the Rearview Mirror | Even though control strategies are taught, doesn’t mean they work |
| Clear out old to make room for new | Field full of dead trees that need to be burned down for new trees to grow |
| Break down reliance on old agenda | “Isn’t that like you? Isn’t that familiar? Does something about that one feel old?” |
| Paradox | Telling client their confusion is a good outcome |
| Feedback screech metaphor | It's not the noise that is the problem, it’s the amplification |
| Control is a problem | How they struggle against it = control strategies (ways they try to control or avoid inner experience). |
| The paradox of control | “If you aren’t willing to have it, you’ve got it.” |
| Illusion of control metaphors | Fall in love, jelly doughnut, what are the numbers exercise |
| Consequences of control | Polygraph metaphor |
| Willingness vs. control | Two scales metaphor |
| Costs of low willingness | Box full of stuff metaphor, clean vs. dirty discomfort |
These clinical materials were assembled by Elizabeth Gifford, Steve Hayes, and Kirk Stroshal
Cognitive Defusion (Deliteralization)
Cognitive Defusion (Deliteralization)Purpose: See thoughts as what they are, not as what they say they are.
Method: Expand attention to thinking and experiencing as an ongoing behavioral process, not a causal, ontological result
When to use: When private events are functioning as barriers due to FEAR (fusion, evaluation, avoidance, reasons)
Examples of defusion techniques
| ‘The Mind” | Treat “the mind” as an external event; almost as a separate person |
| Mental appreciation | Thank your mind; show aesthetic appreciation for its products |
| Cubbyholing | Label private events as to kind or function in a back channel communication |
| “I’m having the thought that …” | Include category labels in descriptions of private events |
| Commitment to openness | Ask if the content is acceptable when negative content shows up |
| Just noticing | Use the language of observation (e.g., noticing) when talking about thoughts |
| “Buying” thoughts | Use active language to distinguish thoughts and beliefs |
| Titchener’s repetition | Repeat the difficult thought until you can hear it |
| Physicalizing | Label the physical dimensions of thoughts |
| Put them out there | Sit next to the client and put each thought and experience out in front of you both as an object |
| Open mindfulness | Watching thoughts as external objects without use or involvement |
| Focused mindfulness | Direct attention to nonliteral dimensions of experience |
| Sound it out | Say difficult thoughts very, very slowly |
| Sing it out | Sing your thoughts |
| Silly voices | Say your thoughts in other voices -- a Donald Duck voice for example |
| Experiential seeking | Openly seek out more material, especially if it is difficult |
| Polarities | Strengthen the evaluative component of a thought and watch it pull its opposite |
| Arrogance of word | Try to instruct nonverbal behavior |
| Think the opposite | Engage in behavior while trying to command the opposite |
| Your mind is not your friend | Suppose your mind is mindless; who do you trust, your experience or your mind |
| Who would be made wrong by that? | If a miracle happened and this cleared up without any change in (list reasons), who would be made wrong by that? |
| Strange loops | Point out a literal paradox inherent in normal thinking |
| Thoughts are not causes | “Is it possible to think that thought, as a thought, AND do x?” |
| Choose being right or choose being alive | If you have to pay with one to play for the other, which do you choose? |
| There are four people in here | Open strategize how to connect when minds are listening |
| Monsters on the bus | Treating scary private events as monsters on a bus you are driving |
| Feed the tiger | Like feeding a tiger, you strengthen the impact of thoughts but dealing with them |
| Who is in charge here? | Treat thoughts as bullies; use colorful language |
| Carrying around a dead person | Treat conceptualized history as rotting meat |
| Take your mind for a walk | Walk behind the client chattering mind talk while they choose where to walk |
| How old is this? Is this just like you? | Step out of content and ask these questions |
| And what is that in the service of? | Step out of content and ask this question |
| OK, you are right. Now what? | Take “right” as a given and focus on action |
| Mary had a little …. | Say a common phrase and leave out the last word; link to automaticity of thoughts the client is struggling with |
| Get off your buts | Replace virtually all self-referential uses of “but” with “and” |
| What are the numbers? | Teach a simple sequence of numbers and then harass the client regarding the arbitrariness and yet permanence of this mental event |
| Why, why, why? | Show the shallowness of causal explanations by repeatedly asking “why” |
| Create a new story | Write down the normal story, then repeatedly integrate those facts into other stories |
| Find a free thought | Ask client to find a free thought, unconnected to anything |
| Do not think “x” | Specify a thought not to think and notice that you do |
| Find something that can’t be evaluated | Look around the room and notice that every single thing can be evaluated negatively |
| Flip cards | Write difficult thoughts on 3 x 5 cards; flip them on the client’s lap vs. keep them off |
| Carry cards | Write difficult thoughts on 3 x 5 cards and carry them with you |
| Carry your keys | Assign difficult thoughts and experiences to the clients keys. Ask the client to think the thought as a thought each time the keys are handled, and then carry them from there |
These clinical materials were assembled by Elizabeth Gifford, Steve Hayes, and Kirk Stroshal
Acceptance
AcceptancePurpose: Allow yourself to have whatever inner experiences are present when doing so foster effective action.
Method: Reinforce approach responses to previously aversive inner experiences, reducing motivation to behave avoidantly (altering negatively reinforced avoidant patterns).
When to use: When escape and avoidance of private events prevents positive action
Examples of acceptance techniques
| Unhooking | Thoughts/feelings don’t always lead to action |
| Identifying the problem | When we battle with our inner experience, it distracts and derails us. Use examples. |
| Explore effects of avoidance | Has it worked in your life |
| Defining the problem | What they struggle against = barriers toward heading in the direction of their goals. |
| Experiential awareness | Learn to pay attention to internal experiences, and to how we respond to them |
| Leaning down the hill | Changing the response to material – toward the fear not away |
| Amplifying responses | Bring experience into awareness, into the room |
| Empathy | Participate with client in emotional responding |
| In vivo Exposure | Structure and encourage intensive experiencing in session |
| The Serenity Prayer | Change what we can, accept what we can’t. |
| Practice doing the unfamiliar | Pay attention to what happens when you don’t do the automatic response |
| Acceptance homework | Go out and find it |
| Discrimination training | What do they feel/think/experience? |
| Mindreading | Help them to identify how they feel |
| Journaling | Write about painful events |
| Tin Can Monster Exercise | Systematically explore response dimensions of a difficult overall event |
| Distinguishing between clean and dirty emotions | Trauma = pain + unwillingness to have pain |
| Distinguishing willingness from wanting | Bum at the door metaphor – you can welcome a guest without being happy he’s there |
| How to recognize trauma | Are you less willing to experience the event or more? |
| Distinguishing willingness the activity from willingness the feeling | Opening up is more important that feeling like it |
| Choosing Willingness: The Willingness Question | Given the distinction between you and the stuff you struggle with, are you willing to have that stuff, as it is and not as what it says it is, and do what works in this situation? |
| Focus on what can be changed | Two scales metaphor |
| Caution against qualitatively limiting willingness | The tantruming kid metaphor – if a kid knew your limits he’d trantrum exactly that long; Jumping exercise – you can practice jumping from a book or a building, but you can step down only from the book – don’t limit willingness qualitatively |
| Distinguish willing from wallowing | Moving through a swamp metaphor: the only reason to go in is because it stands between you and getting to where you intend to go |
| Challenging personal space: | Sitting eye to eye |
These clinical materials were assembled by Elizabeth Gifford, Steve Hayes, and Kirk Stroshal
Self as Context
Self as ContextPurpose: Make contact with a sense of self that is a safe and consistent perspective from which to observe and accept all changing inner experiences.
Method: Mindfulness and noticing the continuity of consciousness
When to use: When the person needs a solid foundation in order to be able to experience experiences; when identifying with a conceptualized self
Examples of techniques designed to increase self as context
| Observer exercise | Notice who is noticing in various domains of experience |
| Therapeutic relationship | Model unconditional acceptance of client’s experience. |
| Metaphors for context | Box with stuff; house with furniture; chessboard |
| “confidence” | con = with; fidence = fidelity or faith – self fidelity |
| Riding a bicycle | You are always falling off balance, yet you move forward |
| Experiential centering | Make contact with self-perspective |
| Practicing unconditional acceptance | Permission to be – accept self as is |
| Identifying content as content | Separating out what changes and what does not |
| Identify programming | Two computers exercise |
| Programming process | Content is always being generated – generate some in session together |
| Process vs outcome | Practice pulling back into the present from thoughts of the future/past |
| ACT generated content | Thoughts/feelings about self (even “good” ones) don’t substitute for experience |
| Self as object | Describe the conceptualized self, both “good” and “bad” |
| Others as objects | Relationship vs being right |
| Connecting at “board level” | Practice being a human with humans |
| Getting back on the horse | Connecting to the fact that they will always move in and out of perspective of self-as-context, in session and out. |
| Identifying when you need it | Occasions where “getting present” is indicated (learning to apply first aid) |
| Contrast observer self with conceptualized self | Pick an identity exercise |
| Forgiveness | Identify painful experiences as content; separate from context |
These clinical materials were assembled by Elizabeth Gifford, Steve Hayes, and Kirk Stroshal
Valuing as a Choice
Valuing as a ChoicePurpose: To clarify what the client values for its own sake: what gives your life meaning?
General Method: To distinguish choices from reasoned actions; to understand the distinction between a value and a goal; to help clients choose and declare their values and to set behavioral tasks linked to these values
When to use: Whenever motivation is at issue; again after defusion and acceptance removed avoidance as a compass
Examples of values techniques
| Coke and 7-Up | Define choice and have the client make a simple one. Then ask why? If there is any content based answer, repeat |
| Your values are perfect | Point out that values cannot be evaluated, thus your values are not the problem |
| Tombstone | Have the client write what he/she stands for on his/her tombstone |
| Eulogy | Have the client hear the eulogies he or she would most like to hear |
| Values clarification | List values in all major life domains |
| Goal clarification | List concrete goals that would instantiate these values |
| Action specification | List concrete actions that would lead toward these goals |
| Barrier clarification | List barriers to taking these actions |
| Taking a stand | Stand up and declare a value without avoidance |
| Pen through the board | Physical metaphor of a path – the twists and turns are not the direction |
| Traumatic deflection | What pain would you have to contact to do what you value |
| Pick a game to play | Define a game as “pretending that where you are not yet is more important than where you are” -- define values as choosing the game |
| Process / outcome and values | “Outcome is the process through which process becomes the outcome” |
| Skiing down the mountain metaphor | Down must be more important than up, or you cannot ski; if a helicopter flew you down it would not be skiing |
| Point on the horizon | Picking a point on the horizon is like a value; heading toward the tree is like a goal |
| Choosing not to choose | You cannot avoid choice because no choice is a choice |
| Responsibility | You are able to respond |
| What if no one could know? | Imagine no one could know of your achievements: then what would you value? |
| Sticking a pen through your hand | Suppose getting well required this – would you do it |
| Confronting the little kid | Bring back the client at an earlier age to ask the adult for something |
| First you win; then you play | Choose to be acceptable |
These clinical materials were assembled by Elizabeth Gifford, Steve Hayes, and Kirk Stroshal
Exercises and Meditations
Exercises and MeditationsPlease feel free to attach specific exercises you have found useful in your work (in general or with specific populaitons). Please do not upload attachments that are essentially full treatment manuals or protocols -- those can be uploaded here: www.contextualscience.org/treatment_protocols.
If you have developed your own exercises and tailored them for specific patients, please share them here so that the larger ACBS community may benefit from your particular take on the work, and in turn, you may find additional exercises of use to you here.
"Writing" Acceptance exercise
"Writing" Acceptance exerciseThis exercise is a fun way to help clients understand acceptance.
1st part: The clinician gives a sheet of paper and a pen to the client and says "I'm going to ask you to write a sentence if you're okay". Then the clinician puts an obstacle (a piece of carton board, for ex) in front of client's eyes and says "Wait a minute, is this annoying you if I put this in front of your eyes? Would you prefer if I'd take it off? Well I'm sorry but I'm going to let it there though. However, as you said you prefer to see while you're writing, I allow you to do everything you want to try to see what you're writing. You can move your head, you can get up... Just do everything you can to see what you're writing. Is that okay? So let's go!"
Usually, after 20 to 30 seconds the client has still not written anything readable because s/he has been too occupied with trying to avoid the obstacle so we stop the first part of the exercise. The clinician then says "How was it? Was it difficult? Have you been able to write the sentence? Can we read it?" Obviously not.
2nd part: The clinician says "Well, I'm going to propose you another approach to help you write this sentence finally. I'm sorry but I'm going to let the carton in front of your eyes again. But this time, I propose you not to try to bypass the obstacle but to concentrate your efforts on writing. Maybe it won't be easy but just do your best to write the best you can so as we will be able to read the sentence."
Generally, the client very quickly writes a sentence that we are able to read and we can debrief then. A possibility is to ask the client to write some action linked to his/her value and to write on the carton the thing s/he tries to avoid (a painful thought for ex). Also: sometimes clients or participants in workshops get the thing during the first part of the exercise (i.e. s/he stops trying to avoid the obstacle and starts writing the sentence).
This is good too because it means they understand the approach by themselves. But it can be also interesting to encourage them to do as much as possible to see while writing so as to make them observe the difference between the two approaches.
ACT EXPOSURES EXERCISE
ACT EXPOSURES EXERCISEThis worksheet provides an Acceptance based alternative to ERP, graded exposure and behavioural experiments. You can download any of our ACT, CFT or CBT resources by visiting http://www.thinkcbt.com and following the free downloads tab. We also welcome new ACT or RFT resources from other therapists. Our ACT, CFT and CBT resources are free to download and share with clinicians and members of the public.
ACT Thought Record
ACT Thought RecordAttached is an ACT take on the traditional CBT thought record. I have used this with clients and also in training workshops to illustrate one of the differences between ACT and CBT; acceptance, present moment awareness, and values vs. the 'struggle' of evidence for and against, and changing thinking.
ACT for everyday life
ACT for everyday lifeDisclaimer: This is a worksheet which is designed to be used by a therapist for therapy purposes only. The therapist using the worksheet takes full responsbility for its use and any impact of it on the client/therapy process.
Purpose of the worksheet: The aim is that the therapist works through the four steps with the client sequentially, you can break these up and divide it over a few sessions. It is most useful for people who are struggling with everyday activities, or activities of daily living (ADLs). This may be because of mood issues or physical discomfort.
Accept, Choose-Commit, Take Action Meditation
Accept, Choose-Commit, Take Action Meditation Tom LavinAcceptance physical exercise
Acceptance physical exerciseOriginally submitted by Josh Hillie:
Attached is an exercise that I transcribed from Dr. Sonja Batten's interview from “ACT in Context podcast #4” time mark 48:20 – 1:04. Overall I have found the podcast to be a great resource and very informative. Thank you to all who are doing this good work!
Important pieces for clinician to be mindful of:
1) It is important to have some kind of therapeutic bond/trust first where the client is willing to have therapist do something a bit odd/unconventional.
2) It is not about creating this grand AHA! moment, but more about the process of getting the client to understand the different ways of responding to their struggles.
3) This exercise does not have to make complete sense to the person at that very moment it was conducted. The clinician can revisit the exercise, and/or parts of it, and tie it in to later in that session, our revisit it in later sessions.
4) Therapist and client can create their own shorthand and sometimes when people can relate to things physically it can make it a little more understandable.
5) Appropriately choose your target for this type of exercise. For someone who has a significant very real trauma history you do not want to work with them to defuse or minimize their experience in anyway. Rather you might choose a medium level target, so maybe not focusing on your client’s thoughts and feelings about the traumatic event itself, but instead come up with examples about how in other ways these struggles are coming up in their lives.
Ex. An Interpersonal violence survivor where intimacy is really difficult: rather than doing this exercise with the actual thoughts, feelings, memories of the specific event itself… but instead some of the thoughts and feelings that show up when they are with their significant other or with other people who get physically close to them and it makes them physically uncomfortable. Focusing on targeting something in the here and now vs. targeting something that is related to the past trauma itself.
Acceptance Physical metaphor via Dr. Sonja Batten: ACT in Context podcast
Materials: small index cards & marker
First: Identify what person is struggling with.
Second: Once issue is identified then ask:
When dealing with ___ what’s the first thing that shows up? Client responds.
Third: When your [insert person’s response] what thought goes through your head?
Fourth: And what shows up next?
Fifth: Continue asking questions until you have 6 – 10 separate index cards with client responses pertinent to the specific struggle that they have identified.
(i.e. Thoughts?, Feelings?, Bodily Sensations?, Images that come to mind?, Memories that show up?, Urges?)
Example Script:
Client identifies struggle with Panic.
When dealing with Panic what’s’ the first thing that shows up?...My chest gets tight.
Clinician: write on index card “chest gets tight”
So when your chest starts getting tight what thought goes through your head?...I can’t take this.
Clinician: Write on a separate index card “I can’t take this”
And what Happens next? I have trouble breathing
Clinician: Writes on a separate card “Trouble breathing”
Sixth: Ask permission.
Clinician: “Would you be willing to do something a little bit odd/different/wacky with me?”
If client agrees “Yes”
Seventh: Set up 2 chairs across from each other (a couple feet apart)
Suggest if they would be open to practicing different ways to responding to these thoughts, sensations, images etc. when they show up.
Eighth: Sit in respective opposite chairs:
Clinician: “I am going to gently toss these cards one at a time over to you and what I want you to do is bat them away or move your body or do whatever you have to do to not be in touch with these cards in anyway. Clinician goes through each card one by one reads it and gently toss it over to the person…take a pause...then read next card…pause…repeat until all cards are read.
Process activity: Take time to process with the person what that experience was like.
Clinician: “How was the experience for you?”
Client: “I was a little nervous at first but I was able to batt them away and it was ok I was able to do something about it”
Clinician: “So as we were doing that do you think you would have been able to do something that was important to you at the same time?” (Adapt that to something that is important to the person that these problems have been getting in the way of)
Ex. Clinician: “Do you think while you were batting those things away could you have____ ? “ ex. done that work presentation?... read that book to your kids?,… had that important conversation with a loved one?
Client: “No, I was too focused on making sure that those cards didn’t touch me.”
Ninth: Gather the cards up with the person and tell them we are going to do this in a different way.
Clinician: “This time I want you to cover your eyes with your hands and try to distract yourself however you can. You are not going actively fight with these things but I want you to not to look at them, not to try to notice what’s going on, and just try to distract yourself as much as you can.”
Clinician goes through each card one by one reads it and gently toss it over to the person…take a pause...then read next card…pause…repeat until all cards are read.
Process activity: Take time to process with person what that experience was like.
Clinician: “What was that experience like for you?
Client: “It was sort of upsetting, I wasn’t doing anything, but after a while I was able to check out and distract myself thinking about what happened yesterday” (or whatever they were distracting themselves with during the activity)
Clinician: “And when you were in that stance would you have been able to ____?” Ex. do that work presentation?... read that book to your kids?,… have that important conversation with a loved one?
Client: “well no because I was focused on just checking out at that moment”
Note: Distraction or numbing emotions, or finding different ways to check out in the present moment, if that is your characteristic, most common, and routine way of dealing with stress or difficult situations, then that is likely to be a problem.
Experiential avoidance: It’s not that avoidance is bad per say, it’s just that when doing so creates more problems, or it can be harmful (i.e. doing drugs). Pervasive way vs. way that someone mindfully chooses to use distraction.
Tenth: Third step in this exercise gather up cards again with the client.
Clinician: “Ask you to remain in the chair with feet flat on the floor and put your arms on your lap with palms facing up in an open welcoming gesture. Would you be willing to try this a third time?"
If yes…
Clinician: "Now I am going to call out each card one at a time and gently toss these cards over to you and I want you to notice what I am saying, be present here in the moment, and keeping you open welcoming gesture can you let the cards come over and do what they are going to do?”
Clinician: goes through each card one by one reads it and gently tosses it over to the person…take a pause...then read next card…pause…repeat until all cards are read. This time the cards might fall on the persons lap, bounce off them, miss them and land at their side. Client’s job is just to be there and be present and in contact with each one of those experiences for however long it’s there.
Process activity: Take time to process with person what that experience was like.
Clinician: “So if you were in this open stance could you at the same time that these cards were coming over to you have been able to____?” Ex. do that work presentation?... read that book to your kids?,… have that important conversation with a loved one?
Client: “Yeah, at least in this stance I could get closer to it. I feel I did a little better than the other times at least.”
Purpose of activity: It is not trying to get the person to have any one particular experience but rather it’s a physical metaphor to help distinguish between the different ways that we can respond when these certain thoughts, memories, feelings, sensations come up.
a) We can try to fight them and take these active measures to control these thoughts, feelings, sensations etc. when they show up.
b) We can try to ignore, dissociate, distract, or numb and not be in touch with what’s going on.
c) Or can you be open and willing to experience whatever is there for however long it wants to stick around for. Without Holding onto it or pushing it away.
Butterfly Exercise
Butterfly ExerciseI wrote this exercise based on the "Thoughts as Butterflies" metaphor found in various ACT materials such as the "Learning ACT" book. I have used it in my ACT group and have recieved positive feedback. Feel free to comment and critique!
Spanish version submitted by Paulina Salles.
Defusion Exercises
Defusion Exercises Joel Guarna10 Cognitive Defusion Exercises +FAQ
10 Cognitive Defusion Exercises +FAQ
✨ Discover a curated selection of 10 cognitive defusion techniques, each crafted to help therapists assist clients in detangling from unhelpful thought patterns.
✨ Plus an FAQ section that addresses common questions, enriching your professional toolkit with clarity and ease.
10 Cognitive Defusion Exercises +FAQ
 .
. 
Airplanes - Defusion
Airplanes - Defusion Danielle PotokarFor he's a jolly good (insert X)
For he's a jolly good (insert X)Another good silly song is "for he's a jolly good fellow" including the "so say all of us". The most fun I've had with it was a client with Schizophrenia and OCD, fused with the idea that people in the shopping mall knew about an incident where he made "obscene" phone sex calls to some girls he was interested in. It was paralysing his ability to go out in public with his friends. He saw himself as a sick pervert. So we sang "For he's a jolly good pervert...." Try it - its almost impossible to get through twice without collapsing in laughter. It has considerably (but not totally) weakened the power of the idea.
Spanish version submitted by Paulina Salles:
Por qué es un buen compañero
Una canción tonta que sirve para esto es "Porque es un buen compañero", incluyendo el "y nadie lo puede negar".
Lo más gracioso que he tenido con este ejercicio fue con un cliente con esquizofrenia y el TOC, fusionado con la idea de que la gente en el centro comercial sabía acerca de un incidente en donde hizo sexo telefónico "obsceno" llamando a algunas chicas que que le interesaban. Estaba paralizando su capacidad de salir a la calle con sus amigos. Se veía a sí mismo como un enfermo pervertido.
Así que cantamos... "Porque es un buen pervertido...." Pruébelo - es casi imposible pasar dos veces sin que se hunda en la risa.
Este ejercicio debilitó considerablemente (pero no totalmente) el poder de la idea.
News of the World
News of the WorldSchool of Fish
School of Fish A cognitive defusion and acceptance exercise including instructions (see attached, pdf format). What it is (from the exercise instructions): "In some ways, our experience of anxiety is like our experience of a school of fish. Imagine a school of fish seen from a distance. What you see is a large, looming, perhaps frightening shape moving through the water. It looks more like a large fish, perhaps a shark, than a group of tiny fish... If we got closer we would see the frightening object for what it is: not an object at all, but several smaller objects occurring in about the same space at the same time. "
A cognitive defusion and acceptance exercise including instructions (see attached, pdf format). What it is (from the exercise instructions): "In some ways, our experience of anxiety is like our experience of a school of fish. Imagine a school of fish seen from a distance. What you see is a large, looming, perhaps frightening shape moving through the water. It looks more like a large fish, perhaps a shark, than a group of tiny fish... If we got closer we would see the frightening object for what it is: not an object at all, but several smaller objects occurring in about the same space at the same time. "
So Who Are You?
So Who Are You?This defusion exercise was posted by Hermann Meyer on November 29, 2006
Here is one of the best I have come accross: "So Who Are You?"
The witnessing of awareness can persist through waking, dreaming and deep sleep. The Witness is fully available in any state, including your own present state of awareness right now. So I'm going to talk you into this state, or try to, using what are known in Buddhism as "pointing out instructions." I am not going to try to get you into a different state of consciousness, or an altered state of consciousness, or a non-ordinary state. I am going to simply point out something that is already occurring in your own present, ordinary, natural state.
So let's start by just being aware of the world around us. Look out there at the sky, and just relax your mind; let your mind and the sky mingle. Notice the clouds floating by. Notice that this takes no effort on your part. Your present awareness, in which these clouds are floating, is very simple, very easy, effortless, spontaneous. You simply notice that there is an effortless awareness of the clouds. The same is true of those trees, and those birds, and those rocks. You simply and effortlessly witness them.
Look now at the sensations in your own body. You can be aware of whatever bodily feelings are present-perhaps pressure where you are sitting, perhaps warmth in your tummy, maybe tightness in your neck. But even if these feelings are tight and tense, you can easily be aware of them. These feelings arise in your present awareness, and that awareness is very simple, easy, effortless, spontaneous. You simply and effortlessly witness them.
Look at the thoughts arising in your mind. You might notice various images, symbols, concepts, desires, hopes and fears, all spontaneously arising in your awareness. They arise, stay a bit, and pass. These thoughts and feelings arise in your present awareness, and that awareness is very simple, effortless, spontaneous. You simply and effortlessly witness them.
So notice: you can see the clouds float by because you are not those clouds-you are the witness of those clouds. You can feel bodily feelings because you are not those feelings-you are the witness of those feelings. You can see thoughts float by because you are not those thoughts-you are the witness of those thoughts. Spontaneously and naturally, these things all arise, on their own, in your present, effortless awareness.
So who are you? You are not objects out there, you are not feelings, you are not thoughts-you are effortlessly aware of all those, so you are not those. Who or what are you?
Say it this way to yourself: I have feelings, but I am not those feelings. Who am I? I have thoughts, but I am not those thoughts. Who am I? I have desires, but I am not those desires. Who am I?
So you push back into the source of your own awareness. You push back into the Witness, and you rest in the Witness. I am not objects, not feelings, not desires, not thoughts. But then people usually make a big mistake. They think that if they rest in the Witness, they are going to see something or feel something-something really neat and special. But you won't see anything. If you see something, that is just another object-another feeling, another thought, another sensation, another image. But those are all objects; those are what you are not.
No, as you rest in the Witness-realizing, I am not objects, I am not feelings, I am not thoughts-all you will notice is a sense of freedom, a sense of liberation, a sense of release-release from the terrible constriction of identifying with these puny little finite objects, your little body and little mind and little ego, all of which are objects that can be seen, and thus are not the true Seer, the real Self, the pure Witness, which is what you really are.
So you won't see anything in particular. Whatever is arising is fine. Clouds float by in the sky, feelings float by in the body, thoughts float by in the mind-and you can effortlessly witness all of them. They all spontaneously arise in your own present, easy, effortless awareness. And this witnessing awareness is not itself anything specific you can see. It is just a vast, background sense of freedom-or pure emptiness-and in that pure emptiness, which you are, the entire manifest world arises. You are that freedom, openness, emptiness-and not any itty bitty thing that arises in it.
Resting in that empty, free, easy, effortless witnessing, notice that the clouds are arising in the vast space of your awareness. The clouds are arising within you-so much so, you can taste the clouds, you are one with the clouds. It is as if they are on this side of your skin, they are so close. The sky and your awareness have become one, and all things in the sky are floating effortlessly through your own awareness. You can kiss the sun, swallow the mountain, they are that close. Zen says "Swallow the Pacific Ocean in a single gulp," and that's the easiest thing in the world, when inside and outside are no longer two, when subject and object are nondual, when the looker and looked at are One Taste.
You see?
© 1999 Ken Wilber
Spanish translation submitted by Ramiro is attached.
Thoughts as Traffic Exercise
Thoughts as Traffic ExerciseThis is an excercise I created for an ACT-based anxiety group. It uses the thoughts as traffic metaphor and invites clients to do a guided cost-benefit analysis of three common responses to distracting traffic (thoughts).
Get Out of Your Mind and Into Your Life--Support Materials
Get Out of Your Mind and Into Your Life--Support Materials
This is a note from Steve Hayes about the book
I wanted to say a little about what we are learning about the impact of Get Out of Your Mind and Into Your Life
We have used or are using the book as part of our protocols in four scientific studies. The book is very flexible -- you can fit it to almost any issue, so these studies are in several different areas.
One study that is now done is Jason Lillis’s dissertation on weight maintenance. It’s a really neat study, and I predict it will get some publicity when it comes out in a journal.
In that study everyone in the ACT condition got a 6 hour workshop on ACT (not really focused on weight – but focused on doing what you value and learning to sit with difficult thoughts and feelings that get in the way). And everyone in the ACT condition also got the book.
When we then asked at the follow up if people used the book we divided up the groups into those who used it very little and those who used it regularly and carefully. We compared that last group (the readers and regular users) to people in the ACT condition who got the workshop but did not use the book much.
(In truth, in other analyses we also compared the frequent readers to the control group, and the effects there were huge, but that comparison includes the workshop in one group and not the other so it is really not as relevant to the question of whether the book itself was helpful).
At a three month follow up, those who read and used the book carefully in the ACT condition:
- Had a higher quality of life
- Were less judgmental toward themselves
- Felt less judged by others
- Were more accepting of difficult thoughts and feelings about weight issues
- Were more successful in living their values
- Had more intrinsic and less avoidant or socially compliant values
All of these folks got an ACT workshop, and the workshop itself had a really big impact – so this was over and above that. Overall (not dividing the group by whether they read Get Out of Your Mind carefully) people in the ACT condition lost more weight over 3 months, lowered their diastolic blood pressure, had better overall mental health, were more distress tolerant, and so on through a long list of good effects. But on top of that the book seemed to make an impact.
Tami Lazzarone has recently completed a randomized trial of the book with 236 teachers and staff in K - 12. At post those who read the book had small to medium improvements in general mental health, anxiety, depression, and burnout. At a 3 month follow up all of these effects were larger -- mostly medium to large. At the process level changes were found in mindfulness, acceptance, and psychological flexibility and these post changes mediated follow up outcomes.
Takashi Muto has done much the same thing with a Japanese translation of the book -- applying it to college students from Japan who are adjusting to life in the US. It is still underway but at post the effects are very good.
Anyway, let me just say this: there are a lot of books out there that say they will help you. It is one thing to say that. It is another to put a book on the line and see, objectively, how it works in controlled studies. So far the results coming in are very supportive.
BUT
How do we get everyone who buys it to read it carefully and to do the exercises? It seems to take that to make a real difference.
But probably a third of the folks who buy it will get bogged down and some will just abandon the book.
That really distresses me, since I know some of those people are suffering and could be helped if they gave the book a chance.
The bogging down may be due to my science geek writing style (I’m learning, but it is hard for me not to talk like a geek after 30 years in the University, even with a professional writer like Spencer Smith helping me). But the other part is this: this is a tricky area!
The human mind does not like being dethroned, and it is hard to use words to rein in the word machine. That is especially true in a non-interactive medium like a book.
But I do think there are steps that can help.
I suggest this if you buy this book:
- Join the list serve ACT for the Public. This is the link: https://groups.io/g/actforthepublic. It’s free. Post to it when and if you get stuck. Don’t abandon the book before you get help with it. Please.
- It is hard to really do the book carefully right off from the beginning. It takes a while to see what it is really up to.
I suggest that you skim the whole thing in a day or two, skipping the exercises and not stopping if you get confused.
Then let it sit for a day or so.
Then if you sense that there may be something of value for you in the book, open it up at page one and read it carefully, doing the exercises as you go. That process will take at least a month. If an exercise or sections bogs you down, put a post-it note there and move on … you can come back later. And you can post an email about the issue on the list serve.
I hope this helps and good luck!
Steve Hayes
Holding the Boulder of Burden - Worksheet for Chronic Pain
Holding the Boulder of Burden - Worksheet for Chronic PainThe attached worksheet, developed by Brandon Scott, has been used as a daily exercise to trigger and harness creative hopelessness for individuals with chronic pain. It has been used to help clients grow into living their life even if the pain exists.
Identifying being 'On-Track' versus 'Off-Track' in session
Identifying being 'On-Track' versus 'Off-Track' in session
I use this a lot with clients who tend to keep derailing the session. It’s incredibly powerful, and it trains defusion, acceptance, contact with the present moment, and committed action all in one simple intervention. (I wanted to put it into ACT Made Simple, but there was no space –so here it is in print for the first time).
To use this strategy, first, you need to agree that you and the client are a team - working together for a specific goal. (Obviously if the client’s goal is to get rid of their anxiety, you can’t agree to that – you just declare your helplessness; admit you don’t know how to do it in any manner that enriches life; and offer them the alternative: to ‘learn how to handle anxiety more effectively so it has less influence and impact over you’.)
So in this case you and the client might agree the goal is to have ‘more successful social interactions’, or to ‘learn how to handle anxiety more effectively so it has less influence and impact over you’, or to ‘increase social life’ etc.
Okay, that’s step one: agree on a goal, and agree you’re a team.
Step two: you say, ‘Now here’s my prediction. I could be wrong, but i predict that throughout this session, every time we start to really knuckle on down to achieving this goal, your mind is going to try and derail us; to pull us off track. And what I’d like for us to do, if you’re willing, is to identify all the different tactics your mind uses to do this; so we can spot them when they show up, and make sure we don’t get derailed by them. Is that okay?’
Step three: Therapist pulls out a large sheet of paper and a pen.
T: ‘So I’m going to write down here every tactic your mind uses. I’ll start off writing for the first few tactics, and then I’ll pass the paper over to you, and you can take over, okay?’
C: Okay
T: So what’s your mind saying now about this?
C: It won’t work.
T: Okay. Let me jot that down. ‘It won’t work’. (As the therapist says it aloud, he also writes down: ‘It won’t work’). What else?
C: This is bullshit.
T: Okay. ‘This is bullshit.’ (As the therapist says it aloud, he also writes down: ‘This is bullshit.’) What else?
C: I don’t see how this will help me.
T: Okay. ‘I don’t see how this will help me.’ (As the therapist says it aloud, he also writes down: ‘I don’t see how this will help me.’) What else?
After writing down five or six ‘derailing tactics’ - such as, ‘this is weird’, ‘but nothing has ever worked in the past’, ‘I won’t be able to do it’, - the therapist hands the paper and pen to the client.
T: So what I’d like you to do, if you’re willing, is each time your mind comes up with one of these tactics to pull us off track, just put a tick by it, so we can see how many times it shows up. Okay? And if your mind comes up with a new tactic I’ll get you to write it down, add it to the list, okay?
C: Well I can do that, but I don’t see how it’s going to help.
T: Okay, now you’ve already got that one on the list, right there: ‘I don’t see how this will help me’ – so can you place a tick by it?
(Client ticks the statement on the list)
T: See how quickly that one showed up? I bet it’s gonna come back at least another 3 or 4 times this session. Any others showing up?
C: Yeah, this is bullshit.
T: And that’s there too, isn’t it? So put a tick next to that one.
(Client ticks the statement on the list)
T: Any others showing up?
C: Yes. (smiling a little – ticks two of the other statements on the list)
As the session continues, every time the client tries to move away from the goal, the therapist calls it out as a derailing tactic and asks the client to write it down. Most clients have a repertoire of about five to fifteen tactics, and the others they come up with are just variants on these basics. At some point, the therapist is likely to need to have the following conversation:
T: Okay, so now let’s get back to that goal we agreed on.
C: There’s no point. It won’t work.
T: Is that one on the list?
C: Yes. (ticks it) But it’s true! It really won’t work!
T: Well, here’s the thing – I can’t guarantee you that it will work. In fact if you ever visit any professional who guarantees you that their treatment will work, I suggest you don’t go back to them, because they’re either bullshitting you or they’re deluded. Go to the world’s greatest surgeon for an operation and she will not guarantee you a successful outcome; she will ask you to sign a consent form in which you acknowledge all the things that could possibly go wrong. So I could show you lots and lots and lots of research on ACT to prove how effective it is with depression, anxiety, addiction, schizophrenia, you name it ... but that wouldn’t guarantee it will work for you. So here’s what I DO guarantee: I guarantee I will do my very best to help you, using the skills and knowledge that I have. I also guarantee, that if we stop the session because your mind says it won’t work, then I will be of no help to you whatsoever. So here we are – your mind is saying this won’t work – shall we let it say that and carry on, or shall we stop the session?
C: Carry on.
T: Great. So can you write down the words ‘But it really is true’ just there on your sheet, in front of ‘This won’t work’ – and put another tick by that thought, and let’s get back to the goal.
The beautiful thing about the ‘off-track, on-track’ strategy is that you are training defusion, acceptance, contact with the present moment, and committed action without even mentioning that this is what you are doing, and with minimal psycho-education – you’re just right into it. Plus, it helps the therapist defuse and stay on track.
Life Line Exercise
Life Line ExerciseThe life line exercise is an experiential metaphor to help the therapeutic dyad discuss and establish the basic ACT principles. It comes from The Art & Science of Valuing in Psychotherapy: Helping Clients Discover, Explore, and Committed to Valued Action Using Acceptance and Commitment Therapy (Dahl, Plumb, Steward, & Lundgren, 2009). This brief summary was put together as a way of teaching ACT for workshops in Sierra Leone.
Lovingkindness Meditation Script
Lovingkindness Meditation ScriptLoving-kindness meditation is like a warm embrace for the mind, one that fits hand-in-glove with ACT. It’s not about pushing away the tough stuff or painting everything with a sunny sheen. Instead, it’s about opening your heart to kindness and caring—first to yourself, then to others—making it easier to handle life’s ups and downs with a grounded sense of compassion. It’s a heartfelt companion to ACT’s journey towards embracing life as it is, with all its thorns and blooms.
Lovingkindness Meditation Script PDF (and instructions)
 .
. 
Meditar
MeditarMEDITAR
MEDITARMind Sort - Initial Draft
Mind Sort - Initial DraftI put this together to help clients with defusion and self-as-context exercises; using small sticky notes or writing directly on it, clients can label their observations/emotions/predictions/evaluations. By writing these and putting them on the paper, it can serve as a direct example of letting go of our mental content.
Let me know what you think and if any additions/revisions might be helpful. I work with clients who experience psychosis, mood fluctuations, and anxiety so that was what I had in mind when I put this together.
Mindfulness for sleep
Mindfulness for sleep
It is a basic insight in ACT that irrespective what body sensations, feelings or thoughts which occupy us, we can accept that and focus on our values and chose our ACTions and behaviour accordingly.
The problem with insomnia is that sleep is not a behaviour, nothing we can “behave” but a state of consciousness. Of course we can use exercises as muscular relaxation, mindfulness focusing on the body, as body scan or breathing which can relax us an increase the tendency to fall asleep. But it is clearly stated e.g. that in body scan we shall not fall asleep but be awake. Focus on body and breath will not led all the way to sleep, because in sleep we don’t experience, at least not normally, neither the body nor the breathing.
But I think there is a mindfulness exercise, which can bring us even closer to sleep.
When we close our eyes we see, so to speak, behind our eyelids lighted and shaded areas.
If we focus on these phenomena exactly as we do in the raisin exercise, that is focus on the seeing of lighted and shaded areas in all minute details and not evaluating or thinking about what we see, it is my experience that sometimes this can lead to more picture like phenomena. And sometimes more dreamlike sequences which can lead into dream sleep and so in to the cycles of sleep.
I have tested this exercise with a few clients, one with pain often preventing sleep, and it worked sometimes.
It is my hope that others in the ACT community will find this simple exercise worth testing and even develop it further.
Jan Pilotti
M.D. Child and Adolescent psychiatrist
B.Sc. Mathematics, Theoretical physics
Örebro Sweden
PS See also the clear and valuable article Lundh, L.G. (2005). The role of acceptance and mindfulness in the treatment of insomnia. Journal of Cognitive Psychotherapy, 19, 29-39. http://contextualscience.org/Lundh_2005
I think the excercise above can be used in the broader setting which the article clearly present.
SMART Goals - improved
SMART Goals - improvedThis is a reworked version of the old acronym that I put to gether for working with Clients. Feel free to use, hope it helps your work and your Client.
Cheers,
Nik
Serene, meaningful living today
Serene, meaningful living today Tom LavinTin Can Monster exercise -- Audio files
Tin Can Monster exercise -- Audio filesAttached is the Tin-Can Monster exercise, which I recorded using the script from Get Out of Your Mind and Into Your Life. This is a really powerful willingness/acceptance exercise.
I recorded separate tracks for each experiential domain (bodily sensations, emotions, behavioral predispositions, thoughts, memories). This enables clients to repeat tracks to cycle through as many experiences in a domain as they'd like before going on to the next domain.
To go through the whole exercise just once takes a fairly long time (45 min) but people can do this acceptance work in smaller chunks over time. To download the tracks, you must first LOGIN to the site (and be a current paid member) & then when you click on the link & the dialog box appears, click "SAVE" not "play."
Values Exercises
Values Exercises80th Birthday Exercise for Values Exploration
80th Birthday Exercise for Values ExplorationOne of the classic ACT techniques for exploring values is the “imagine your 80th birthday” or the “imagine your funeral,” exercise. There are many ways to do this exercise. Attached to this page is a script showing one example of how to do this. (Be sure to be logged in with a current membership in order to download it). Enjoy!
80th Birthday exercise - therapy homework version
80th Birthday exercise - therapy homework versionThanks for creating this Doug.
I needed to give a version of this to a client this week who wants to do the writing work at home, so I edited your original to suit that format and have uploaded it here.
Feel free to offer it to your clients who like doing homework!
Batteries Exercise: Alternative to Life/Values Compass
Batteries Exercise: Alternative to Life/Values CompassThis is an alternative to the Life/Values Compass exercise and can be used to organize behavioral activation efforts.
I have used this as a metaphor when talking with clients about issues that are otherwise a bit abstract: helping connect them to the contingencies in their natural environment. Several clients have appreciated the metaphor as a simple and common language for having this discussion.
Attached, you can find it in exercise form. I would recommend doing this after you have done some other values assessment/clarification so the client has specifics in mind for each valued domain.
Digital Values Compass Tool
Digital Values Compass ToolOur Life Compass Digital Tool is here to aid ACT therapists in steering clients towards their true north. This interactive online resource simplifies the process of identifying and connecting with personal values, serving as a navigational aid in the therapeutic journey. It's an excellent addition to any ACT toolkit, providing a dynamic way to enrich sessions and empower clients' self-discovery and committed action.
→ ACT Life Values Compass Digital Tool
Trying On a Value
Trying On a ValueThis exercise is a good one for helping clients who do not have a strong sense of their values. Rather than needing to 'know' which value is important to them in order to behave, is it possible to behave for a while to learn from direct experience how it feels to a) commit to behaving consistent with a freely chosen value, and perhaps b) learn over time which values may have meaning for the person? Some work with the client around this issue (e.g., willingness, defusion/letting go of 'needing' to know the answer) will be helpful. My experience is that it's a good idea to assign this as homework for an extended period of time -- at least a few days, a week or two, or longer if possible -- to help the client build up a longer history of behaving consistently with this value before coming to any 'decisions' about continuing to move forward in the direction of that or another chosen value.
Two Sides of the Same Coin worksheet
Two Sides of the Same Coin worksheetUse this worksheet to demonstrate the two sides of the same coin metaphor. Print each slide on one side of the same piece of paper and cut out the circle. Have the client fill out their top 5 most painful internal experiences on one side and their top 5 most important values on the other. Discuss the relationship between the two sides and how you can't have one side without the other. Ask the client to turn the "painful" side up and then "get rid" of it - hide it, push it away, rip it up. Then discuss how trying to push away our painful experiences also results in pushing away our values.
Values Clarification App
Values Clarification AppI wanted to share this little gem with the greater ACT community. The Forstara Personal Values Sort for iphone and android (based on Miller,C’de Baca, Matthews, and Wilbourne's card sort exercise) has been a great way to get clients exploring their values. It takes the somewhat cumbersome task of the card sort and makes it a simple exercise anyone can complete on a smart phone in a few minutes.
Please note, the app listed above is no longer available but another has been suggested if it is of use:
Values Discovery by PanPlus Global, Inc. It’s a card sort app. https://play.google.com/store/apps/details?id=com.Pinnguaq.PPLegacyCards&hl=en
Values List & Interactive Tool
Values List & Interactive ToolI've created a downloadable Values List PDF and an Interactive Online Tool to help your clients pinpoint what's truly important to them.
These easy-to-use resources are great for guiding clients through ACT values clarification, whether as part of homework or during live sessions via screen sharing.
They're practical, straightforward, and ready to be integrated into your work. Give them a try and see how they can support your clients' progress!
→ Values List & Interactive Tool
. .
Virtual Values Card Sort
Virtual Values Card SortPlease watch the video below (https://www.youtube.com/watch?v=U4vbz8BPS0M&feature=youtu.be) that explains the virtual values card sort and then have a play around with the PowerPoint file attached that contains the cards.
Please feel free to adapt, evolve and share the virtual values cards so that they are helpful to your context and so that other people may benefit from them too.
Please contact me at: drrichardcoates@gmail.com if you have any queries. I'd also love to hear how you get on with using them.
The virtual values card sort was a result of values-based behaviour of 'creativity, connection and learning.'
I hope they can be helpful and accessible to everyone, everywhere.
Warm wishes
Richard
Dr. Richard Coates
Clinical Neuropsychologist
UK
What Can I Control Exercise
What Can I Control ExerciseThis is an exercise adapted from Russ Harris's ACT Made Simple (Chapter 9, Drop The Struggle) as an exploration of the areas that we cannot control and developing the ability to control what we can. I ask the client to carefully circle only those phrases that describe what we can potentially control. Once they circle at least nine different phrases we discuss and process their choices. This becomes a teaching tool for exploring the concept of dropping the struggle. I usually will discuss the wisdom of the Serenity Prayer and how our work together will involve identifying and relinquishing control of what we cannot control so that we can develope (psychological flexibility) skills for what we potentially can. Whether or not the client circles incorrect responses, it tends to open the door for exploration and discussion.
Support Materials and Worksheets
Support Materials and Worksheets ACBS staff100+ ACT Journal Prompts
100+ ACT Journal PromptsElevate your clients' reflective practice with our expansive collection of over 100 ACT-themed journal prompts. Designed to inspire deeper self-exploration and align with core ACT principles, this generator is an invaluable tool for therapists seeking to enrich their clients' homework and session work. It’s a perfect resource for sparking meaningful insights and facilitating personal growth, available at your fingertips.
→ 100+ ACT Journal Prompts
ACT brief handouts for clients
ACT brief handouts for clientsI've put together a few handouts for students at the University of New South Wales, Australia. Whilst they were originally designed with students in mind the content is relevant for older adolescents to adults. Topics include: stress and anxiety, low mood / depression, relationships, mindfulness meditation, healthy lifestyle / choices with awareness, "getting unhooked from difficult thoughts" and writing oneself a letter from the future. They are intended as a brief reminder of workshop material (or session discussions) or to be used as a stand alone summary of skills. Feel free to share as appropriate.
ACT Change Plan
ACT Change PlanThis form is a way to list values, things that can't change, and things the client is willing to commit to. This is good early in treatment (when the client is coming with the intent to "get rid of" something.
Defusion Worksheets for Clients
Defusion Worksheets for ClientsSeveral members have shared Defusion worksheets to use with clients.
From Amy S. House, Ph.D. - I made up this defusion worksheet and wanted to share. I’m sure there are other similar ones out there but I couldn’t find just what I wanted so I made this. The worksheet walks clients through just a few well-known defusion strategies, with some self-compassionate perspective taking thrown in. I hope the worksheet will be helpful for some of you and your clients.
Amy's Worksheet "Noticing and Working with thoughts" is attached below.
Bartosz Kleszcz has translated Amy's worksheet into Polish. This translated version is also attached below.
Lior Gilad has translated Amy's worksheet into Hebrew. This translated version is also attached below.
Debbie Sorensen, Ph.D. shared - "I have also struggled to find a thought awareness worksheet that was exactly what I wanted before - and have created one myself, too. I'm attaching it here...in case it's helpful to anyone who wants to draw from multiple versions." Debbie's worksheet is attached as both a word and pdf document below.
PDF Values Cards Document
PDF Values Cards DocumentSeveral people got in touch asking for the PDF values cards doc we have stored, so please see attached. All cards on all pages are aligned so once printed you should be able to carefully cut several sheets at a time (if you've got a decent cutting tool). Credit to Paul Flaxman, who originally shared these cards with myself and colleagues. We just aligned them all on a PDF for ease of producing card decks!
Also, just to say, I would not see these a an alternative to the Values Conversation Cards mentioned in the original thread by Joe and developed by Louise Hayes. I find these to be a great resource and, personally, I use these in quite different contexts to the contexts in which I would typically use the attac hed.
Finally, for anyone who a) has not seen them, b) works with younger clients and c) might be interested, we worked with the charity 1625-Independent People to develop a DNA-v based tool kit, which is also in the form of a card deck. We make no cash on sales and all proceeds go to back into this fab charity (just to be clear!) so I share these here as - bias as I may be - I think they are really cool. Here's the link: The DNA-V Toolkit - A card pack for using ACT with young people : 1625 independent People (1625ip.co.uk)
Shared on 9/11/2021 by Duncan Gillard
The Happiness Trap - Support Materials
The Happiness Trap - Support MaterialsThere is now an entire website full of support materials for The Happiness Trap. Please visit the website for the book.
I have also attached the introductory chapter below.
The Happiness Trap is unique amongst ACT books in that it is the only one that has been written for EVERYONE - therapists, coaches, housewives and astronauts, regardless of whether or not they have ‘mental health issues’ - which also explains ACT in a simple, easy-to-understand manner, without any technical language, or a battery of worksheets.
It is increasingly used as a resource by both therapists and coaches - not only to use with their clients, but also as a way of learning the theory and techniques of ACT in a simple, clear and entertaining manner.
Tom Lavin, MFT, LCADC, ACATA: "Live Better" Worksheets
Tom Lavin, MFT, LCADC, ACATA: "Live Better" WorksheetsWorksheets are designed for universal use and accompany the “Live Better” psychoeducation video series found here.
To access class worksheet, please click on class title below.
Tom Lavin, MFT, LCADC, ACATA: The First Step Workbook
Tom Lavin, MFT, LCADC, ACATA: The First Step Workbook"The First Step Workbook" is designed to support people in becoming more fully aware of how their lives have been affected by the use of mood altering chemicals.
The workbook is often most useful when a person takes time to thouroughly respond to each question and then share their responses with a trusted therapist, group, mentor, or sponsor.
After completing the workbook some people decide they want to make significant changes in their lives.
Values Compass pictures
Values Compass picturessee attachement - & feel free to change it as you like - one is a word doc. & then a jpeg
Values Driven Treatment Goal Development Activity
Values Driven Treatment Goal Development ActivityThis is a treatment goal planning activity that I'm using that I really like. I had been using a values sheet with the teens I work with to help them get in touch with sources of meaning in their stimulus-overloaded, introspection-devoid lives. I love how values are the language of the spirit that lend nobility to our lives and work for Evangelical Fundamentalists as well as stalwart atheists. I'd also done a life domain wheel (like life compass) some years ago as a self esteem development tool for teens though it had too much detail to capture their interest. (That I've found such similar ideas and tools in ACT is very cool). Anyway, I took the 80th birthday/be at your own funeral activity, combined it with the values sheet and life domain wheels to come up with a way that helps people identify highly personally relevant treatment goals. (I'm not too computer savvy so it's not that nice to look at; but it works).
When Clients Can't (or Don't Want to) Connect With Thoughts
When Clients Can't (or Don't Want to) Connect With Thoughts
Russ Harris has shared a free eBook on a topic that comes up often in ACT training: When Clients Can't (or Don't Want to) Connect With Thoughts.
When logged in, you will find the eBook attached below.
Visual Aids
Visual AidsThese are images that may prove useful in the delivery of ACT. They are in PDF format to allow for clear and accurate printing. Individuals are free to use these in their research and practice, but please note that the images are copyright © Steven C. Hayes and are not to be used in commercial publications without written permission. The images come from multiple sources. We will upload this info a little later
ACT Related Illustrations
ACT Related IllustrationsThe content of the illustrations are as follows:
(A) Illustrates some of the problems engendered by control/avoidance/non-acceptance
(B) Compares and contrasts the medical model vs. the ACT model of psychopathology (including the importance of distinguishing means vs. ends in psychotherapy)
(C) A chart containing multiple examples comparing the behaviorist model vs. cognitive model of causation (i.e., do thoughts really cause behaviors?)
(D) A visual depiction of cognitive defusion
(E) Some illustrations that speak to the approach-avoidance conflict associated with willingness
ACT-illustrations (+50!)
ACT-illustrations (+50!)Hi all,
For our Time to ACT! book an illustrator made +50 illustrations for several ACT-exercises and Metaphors (for all ACT-components). Below you will find a link to these illustrations; they are
distributed under the creative commons licence CC-BY-NC; which means that they can be used for free if correctly cited and are not used for commercial purposes.
https://www.actinactie.nl/time-to-act-illustraties/
Warm regards,
Tim Batink
Compass-in-a-card
Compass-in-a-cardI use this cards to work with values. Usually we write short sentence with the chosen direction in the back side, so the client can carry the card around.
Hexagon Models
Hexagon ModelsHexaflex image in a word document. Can be "ungrouped" and modified for use. This is a hexaflex (Hexagon Model of Psychological Flexibility) image that I generated in Word based on the image found in the Practical Guide. It took FOREVER, so I figured it might be worth posting. It IS modifiable if you right or control click and "Ungroup" into the shapes and text boxes I used to make it. Hope this is useful to someone! --- note added later by Steve Hayes: I've also posted two images that can be placed into documents. One is the Hexaflex model, and a related model of psychopathology. These are MS office "png" images but are not modifiable (the originals are in CorelDraw). By the way, we deliberately placed these Hexaflex images in multiple places -- including the list serve -- so that no copyright would be enforcable on them by publishers. If you need a citation, however, an easy one is Hayes, S. C., Luoma, J., Bond, F., Masuda, A., and Lillis, J. (2006). Acceptance and Commitment Therapy: Model, processes, and outcomes. Behaviour Research and Therapy, 44, 1-25.
Mindfulness and Neuroplasticity - client education visual aide
Mindfulness and Neuroplasticity - client education visual aideI use these 2 diagrams to teach clients re how they can train healthier brain pathways through regular practice of mindfulness exercises, as discovered by recent neuroscience research. I usually give them to clients as a single A4 handout, with one of the diagrams on the each side of the sheet.
Functional Diagram of the Brain - BEFORE Mindfulness Training
As a result of our Western-style education system, the thinking centres of the brain (memory, imagination, planning, logic, problem-solving) are highly developed, but the attentional centre (i.e. the prefrontal cortex and its various connections, "the CPU of the computer") is relatively underdeveloped, and the emotional centres are relatively poorly regulated.
As a result, clients can easily get caught in dysfunctional "brain loops" - e.g. a loop between the imagination, emotion and planning centres of the brain results in worry/anxiety ; a loop between the memory, emotion and imagination centre can result in depressive ruminations). The attention centre is often not strong enough to interrupt the loop and redirect attention elsewhere.
Functional Diagram of the Brain - AFTER Mindfulness Training
8-12 weeks of regular practice of mindfulness exercises results in increased size and strength of the "CPU" and its connections (presented in a rather exaggerated fashion in the diagram!) and some decrease in size of the emotion centre (more specifically, the amygdala which is the source of most of our 'unpleasant' emotions).
As a result, when the client notices she is starting to worry or ruminate, she can use her strengthened attention centre to break the loop and redirect attention in more workable directions e.g. committed action based on values.
The 5 small pictures on the right represent the 5 senses (i.e. the 'inputs to the computer') and the 2 pictures on the left represent the 2 main outputs , i.e. action and speech.
Submitted by Dr Kingsley Mudd MBBS, BMedSci, FRACGP, Townsville, Qld, Australia
(The attachments below are only viewable and downloadable for current, paid ACBS members.)
The Lotus and the Swamp
The Lotus and the SwampThis is a visual metaphor/worksheet based on the ancient Hindu and Buddhist metaphor of the lotus flower.
I think it is fairly self-explanatory. I find it particularly useful for highlighting the fact that our painful thoughts/feeling are inextricably linked with our values and goals, and our pain must therefore be embraced if we are to create a rich, full and meangful life. The swamp mud provides the nutrients and fertiliser from which the lotus arises. In the same way, you can't have love without pain, courage without fear, creativity without some contact with "the dark side", and so on.
You can't have the beautiful, pristine, magnificent lotus flower if you don't have the dark, murky, filthy mud of the swamp underneath!!!
Submitted by Dr Kingsley Mudd MBBS FRACGP, Family Physician, Townsville, Qld, Australia
Thought Cards
Thought CardsA set of cards, each presenting a typically encountered thought. The majority are 'unhelpful', with a few more 'helpful' ones thrown in to break up the task. Useful for when a client is so fused they can't actually verbalise what they are thinking - they can flip through and choose the thoughts they recognise. Original artwork helps each thought stand out. Instructions/suggestions for use are provided too.
Available to download and print from our website:
Values Cards for youth and adults
Values Cards for youth and adultsFor a couple of years now I have been training adolescent values by using printed cards to facilitate conversations.
I had been trying to have them published professionally, with the hope of donating any profits to charity; however, my attempts at finding a publisher who could produce them for a reasonable cost have failed (other types of kids counselling cards are around $50 AUS).
So, I decided to make them free, by creating them without the professional graphics and posting them for free.
With Lisa Coyne's help they are now ready and available on ACBS.
You can find them here - http://contextualscience.org/louise_hayes039_training_page
ACT folks tell me that the physical properties of having about 10 cards laid out on the desk seems to take the pressure off young people when talking of values. They get some choice in the conversation, and they can focus on the cards rather than the therapist. Somehow it seems to facilitate values dialogue. And the most useful values discussions often come from unexpected questions, like my personal favourite, "do you prefer blending in or standing out?"
I have had pretty good feedback from people who have attended my training that they work well in the clinic with young people as well as adults.
I hope they are useful.
You just need to download them and have them printed and cut up by a print shop.
kind regards, Louise
ACT Relevant Books, Films, Songs, Poems, and Quotes
ACT Relevant Books, Films, Songs, Poems, and QuotesBelow are lists of books/stories, films/videos, songs, poems, and quotes relevant to ACT.
A Dash Of Lime..A Bit Of Honey
A Dash Of Lime..A Bit Of HoneyHere is a short film in Hindi ( with English subtitles) with an ACT relevant theme like living in the Present, Acceptance etc..
Synopsis from Youtube:
------------------
The story is about Anindya who is on the verge of committing sucide. But the very night he has a surreal encounter with life and death personified. Will anindya change his decision???
A life of being right versus a living life - a short scene
A life of being right versus a living life - a short sceneThis final scene (around 20 min, subtitled in english), on website below, of indian movie Mohabbatein won best scene of year 2000. I think it illustrates in a simple dialogue between son-in-law and father-in-law, a life with pain/value versus a life without pain and changes.
In my humble opinion, I don't think the complete movie is worth watching, the best scenes being the ones between son-in-law and father-in-law. Plus, it is easy to understand this scene even if we didn't see the complete movie. Megha is the dead daughter. The beginning of this sequence is a little slow but climax will come. It is after 4 min that it is starting to unravel...... and around 10 min when the father talks to his students.
Indian movies have often this naïvely sentimental way of presenting things and often emphasize intensity of feelings by spectacular settings (nature is often present ---- thunder, lightning, strong wind, sunrays, etc.....).
For a relax way of learning ACT in life!
Cristel
ACT Animation - M!ndi on youtube
ACT Animation - M!ndi on youtubehere's a link to M!ndi's animated story on youtube "Struggling with Internal Hijakers?"
+ M!ndi's message packs!!!
The attached files are the messages that you receive with the iphone app and desktop versions of M!ndi.
We hope you find them useful. Please feel free to use with your clients. And direct them to M!ndi's web page..
NeLi and James
ACT Onscreen: Films for Clients
ACT Onscreen: Films for ClientsThis section of ContextualScience.org is for practitioners looking for a film to prescribe to their clients. Along the lines of the suggestions made in Rent Two Films and Let's Talk in the Morning, by John and Jan Hesley or "The Motion Picture Prescription: Watch This Movie & Call Me in the Morning - 200 Movies to Help You Heal Life's Problems", by Gary Solomon. I've found many films contain moments or plot turns that are highly suitable as metaphors for ACT processes. I invite the ACT community to contribute to this resource so we can help our clients and learn from each other.
Here's Jason Luoma's suggested ratings format and modifications to my original proposal. Thanks Jason!
At a recent lab retreat, Steve's lab came up with the idea of each movie receiving a hexaflex point rating. This similar to the 0, 1, or 2 two thumbs up from Ebert and Roper, but instead goes from 1 to 6, depending upon the number of ACT processes illustrated. The ultimate prize goes the person who can come up with a movie that illustrates all six ACT processes. Will YOU take up the challenge? It can come from multiple scenes in one movie. The ultimate challenge would be to identify one scene that illustrates all six processes. Go fot it!
I'd suggest when you review a movie, at the start you give it a hexaflex rating according to how many processes the movie illustrates.
The six processes are:
- Contact with the present moment
- Acceptance
- Defusion
- Self-as-context
- Values
- Commitment
For example, a movie that illustrates four of these proceses would get four hexaflex points! So as a format for ratings, I'd suggest the following:
- Film name
- Number of Hexaflex Points
- Character, moment or plot point
- ACT principle illustrated and which processes it involves.
Also you might want to put the number of hexaflex points in the title section.
Julian: Here's an example (one of my favorites ;-)):
- The Matrix
- 1 Hexaflex point (but see Camilla's additional point below)
- Neo, the Keanu Reeves character, is asked to choose between the red pill or the blue pill
- Choosing and Willingness - sometimes you can't know the outcome before you choose. Are you willing to have the consequences of choosing and just choose?
Here's Jason's example:
- Indiana Jones and The Last Crusade
- 3 hexaflex points
- When Indiana is just about to get to the holy grail, he finds himself stuck at the edge of a seemingly bottomless chasm. He reads a riddle that suggests that the only way to get across the chasm is to take a leap of faith. So he steps out into mid air, seemingly to fall to his death. Instead, he finds that there is actually a hidden bridge that was built to blend seemlessly into the backdrop of the chasm and his step lands on terra firma. Whew!
- The scene illustrates committed action, in that Indiana takes a step towards his quest even when unsure of the outcome. It illustrates willingness/acceptance in that the move is leadp of faith, requiring him to make room for his fear. And it illustrates defusion in that while his mind tells him he is going to fall to his death, he is willing to suspend that judgment, and when he actually steps out into a seeming void, he finds that this was an illusion.
To contribute your film, click on add child page below. In the Body section of the Edit page, include the following:
- Your Film
- Number of Hexaflex points
- The part where the character says something
- ACT Principle represented
Simple as that!
Hope we have a lot of fun and learning with this,
A Beautiful Mind - 4 Hexaflex points (acceptance, defusion, values, committed action)
A Beautiful Mind - 4 Hexaflex points (acceptance, defusion, values, committed action)- Beautiful Mind
- Pretty much the whole thing. The main character, John Nash (Nobel Prize winner in economics), has schizophrenia and despite active hallucinations and delusions, he chooses NOT to be on antipsychotic medication (side effects are blunted affect and he isn't as clear in his genious mathematical ability). Nash chooses to just let his hallucinations be present and not to let his behavior be guided by belief in them as literal "truth". In turn, they follow him around for the rest of his life; a vital life full of meaningful experiences with his wife and his work.
- ACT Principles: acceptance, willingness, defusion, choice and valued action.
A Beautiful Mind - Comment submitted by Steven Hayes on February 12, 2006.
We all have our little girls following us around, hallucination or no. We need to learn to acknowledge them and then, sad though it is, to learn to be silent if it is costing us what we value to do otherwise.
You could do a lot worse when asked to explain ACT that simply to say "it is teaching folks how to do A Beautiful Mind thing with their own struggles"
- S
Steven C. Hayes, University of Nevada
About Schmidt (2002)
About Schmidt (2002)This movie is all about psychological inflexibility. Warren Schmidt (magnificent played by Jack Nicholson) is a man who's identity is built around his work (he is vice-president of an insurance-company). The film starts with his retirement's party: beautiful words spoken, compliments given..., but only one day later he discovers that he's not welcome anymore at the office, and all his work ends up in a garbage can. Soon after that his wife suddenly dies, and although he feels like a prisoner in his marriage for over 42 years, he loses in a short time everything.
From that moment on his orderly life becomes chaotic and impulsive. He start's traveling with his king-size camper, visiting his daughter, finding out that he has never connected to her because of his work and now she doesn't need him anymore. He's afraid of intimacy and is running away from it or he spoils the moments were it's growing. He can only connect to his "true" feelings in the letters to Ngudu, a foster-child in Africa he has adopted for $22 a month, and to whom he writes from time to time (although the child is to young to read his letters).
It is there where psychological flexibility starts, painfully facing the life he lived. I would say a movie about self-as-content, experiential avoidance, lack of values and impulsive behaviors.
Must-see!!!
American Beauty
American Beauty- American Beauty
- Much of the movie can be cast into terms relevant to clinical work with ACT. I often refer to people having an "American Beauty" moment in which they wake up one day and realize how their lack of mindfulness/life momentum has led them very far off-course from a path consistent with their values (like the Kevin Spacey character and others).
- ACT Principle: There are numerous illustrations of mindfulness (and lack thereof) and the cost of experiential avoidance in the behaviors and choices of the characters.
American History X - Hexaflex points: 6
American History X - Hexaflex points: 6- American History X
- 6 hexaflex points
- I think this film could be seen as illustrating all the Hexaflex points:
Contact with the present moment- (this is the one I'm least sure about): there is a scene between the main character (white supremacist Derrick Vinyard) & a fellow prisoner (Lamont), who is black, where Derrick manages to make contact with the humour of Lamont's impression of 'angry sex' despite his deeply ingrained mind story of racial hatred.
Acceptance - two scenes stand out here: the first is when Derrick is recovering in the prison hospital after being raped & he is visited by his old school principal, Dr Sweeney, & for the first time in the film Derrick accepts any other emotion than anger, which is demonstrated by his crying (sadness) & acknowledgment of not knowing what to do (uncertainty). Second example is toward the end of the film when Derrick is asked by the police to help deal with the inevitable inter-racial tensions following an attack &, despite Derrick not wanting to get involved, he reluctantly agrees to help as he sees that he must accept his responsibility for the situation.
Defusion - the whole of the film post Derrick's release from prison is about him defusing from his racist beliefs & trying to achieve the same with his younger brother, Danny.
Self-as-content: Similarly, Derrick & Danny both identify strongly with their white supremacist beliefs throughout most of the film, even to the point of tattooing swastikas on to themselves, adopting the skinhead hairstyle, indulging in racist attacks etc. It is only when they can stand back from this view can they find compassion & a flexibility of mind.
Values: during the previosuly mentioned scene when Derrick is in the prison hospital & is visited by Dr Sweeney, he is asked by his ex-principal "Has anything you've done made your life better?" This is clearly a turning point for Derrick who then accepts Dr Sweeney's advice & acts on it by reading the books he has brought him. He also defuses from his racist view of the man & sees his true worth. His belief in his racist values is also undermined when he sees the leader of the white supremacist gang trade drugs with a Mexican gang - he remains true to his values at that point by leaving their protection, but pays a heavy price when he is then raped by the gang members.
Commitment: On leaving prison Derrick commits to turning his back on his racist way of life & behaving truer to his values of being a good example for his younger brother & trying to do his best for his family (with whom he previously fought & bullied).
Another movie with ACT-like messages is Happy Feet
Another movie with ACT-like messages is Happy FeetSurprisingly and overwhelmingly ACT-consistent...Happy FeetI don't have time right now for the whole hexaflex thing but I just saw Happy Feet. For those of you who don't know, it is an animated Disney film with penguin stars. It was great, and there are wonderful messages in there about acceptance and valuing. It would be great to watch with children to spark discussions about all kinds of things from prejudice to global warming. Plus, it was just really darn cute!
I should note that there are definitely some stereotyped characters in this movie. If anyone is offended by those kinds of things, be forewarned. Still, I think that the message far outweighs that stuff.
Amy
Buck (2011)
Buck (2011)The film focuses on the life of a current day horse handler/cowboy living his values while acknowledging past abuse, even drawing on what that experience got him in contact with and utilizing it. Acceptance, committed action and present moment focus are all over the place.
Click
ClickCrash (defusion. commited action and values)
Crash (defusion. commited action and values)There is not a particular scene in Crash that I think demonstrates the issues of values and defusion, I think as a therapist you could use the film as a whole to talk about values and defusion (evaluation, that is).
The movie is about racism in Los Angeles, how ordinary people do nasty things to each other on the basis of prejudice and how people make choices in the service of their values and in the service of fear.
To start with evaluation: You could ask a client who are the bad guys and who are the good guys. The nice thing about the movie is that all the characters are doing things that hurt other people and that help other people. So there is no good or bad. And you could talk about how prejudice is something we all do, because of relational framing. And that you can ACT in a different way.
The aspect of values and commited action is closely related. You can talk with a client about the characters: When do they move in the direction of their values and when are they moving in a opposite direction. And relate this to values that clients have for themselves.
Jacqueline
Elizabethtown
Elizabethtown1. Elizabethtown
2. Number of Hexaflex Points :3
3. When Kirstin Dunst says to Orlando Boom: ' ok, you failed. You failed, you failed, you failed etc' ; whole movie is about living a values-led life, in the present
4. Nice example of defusion through repetition as per Milk, milk, milk
However,example of self as content when Dunst is fused with what it means to be 'a Claire' (ie the 'substitute' person).
I ♥ Huckabees
I ♥ Huckabees- I ♥ Huckabees
- Pretty much the whole film, but especially the conversations between the Dustin Hoffman and Anjelica Huston characters.
- ACT Principles: Live a rich, meaningful life and what has experiential avoidance cost you?
Indiana Jones and The Last Crusade: 3 hexaflex points (acceptance, defusion, committed action)
Indiana Jones and The Last Crusade: 3 hexaflex points (acceptance, defusion, committed action)- Indiana Jones and The Last Crusade
- 3 hexaflex points
- When Indiana is just about to get to the holy grail, he finds himself stuck at the edge of a seemingly bottomless chasm. He reads a riddle that suggests that the only way to get across the chasm is to take a leap of faith. So he steps out into mid air, seemingly to fall to his death. Instead, he finds that there is actually a hidden bridge that was built to blend seemlessly into the backdrop of the chasm and his step lands on terra firma. Whew!
- The scene illustrates committed action, in that Indiana takes a step towards his quest even when unsure of the outcome. It illustrates willingness/acceptance in that the move is leap of faith, requiring him to make room for his fear. And it illustrates defusion in that while his mind tells him he is going to fall to his death, he is willing to suspend that judgment, and when he actually steps out into a seeming void, he finds that this was an illusion.
Inside Out
Inside OutInside Out - Disney/Pixar
It's hard to isolate any particular ACT relevant scenes - the whole movie was an animated version of ACT come to life! Essentially, Riley (11 year old girl) has to learn to live with a new life that her parents have chosen, leaving her old, highly valued life behind. She has 4 emotions controlling her from inside her brain - Joy (the dominant emotion up to this point), Sadness, Anger and Disgust.
Due to the new experiences of distress, loneliness, disappointment and anger, Riley starts to experince 'negative' emotions for the first time and Joy has huge problems accepting this. She fights desperately and valiantly to prevent Riley experiencing Sadness, but eventually learns to accept that Sadness is a valid emotion and has a useful part to play. Riley is eventually able to include Sadness, for the old friends and life she has left behind, while building a new life in her new town, heading back towards her values.
Plus, it's really sweet, funny and engaging.
It's a wonderful life (5 ACT processes)
It's a wonderful life (5 ACT processes)It’s a wonderful life: ACT processes
1. Contact with the present moment (and lack of): This I think is illustrated through George’s suicide attempt. He believes he has lost the money from the Building and Loan and that he his a failure and that now Potter will win (and it will be his fault). Such is George’s sense of dejection and impending rejection by the towns people that he attempts to escape by jumping from the bridge. Not only does George not want to be in contact with the present moment, but he wants to have never been born at al.
Georges decision at the end of the movie to have his life back demonstrates this beautifully I think. Before he realises the towns people have all come to help him out he takes his life back and contacts the present moment (which at that point is one of uncertainty over the missing money). He allows himself to be present and open to their criticism and the consequences of losing the money to find their love, help and support instead
2. Acceptance: This is perhaps demonstrated by George’s desire to keep living with the uncertain consequences he faces. I think the key message George takes from Clarence is that it is that upsetting things happen AND it's a wonderful life.
3. Defusion/fusion. Not explicit, but George does not explicitly decide that he has not let the towns people down, it is possible that he stills feels this way, but he has defused from it enough to allow himself to be present with the towns people and the consequences of losing the money.
4. Values: George values helping the town people. He values his family, he values making the town a better place and protecting it from exploitation from Potter
5. Commitment: In the movie, George not only values his values but is actively committed to not letting Potter exploit the town for his own financial gain. His actions are focused on changing the physical (i.e. fighting against Potter- a workable change agenda)
6. Self-as-context: not sure about this one, might there be a sixth process hiding in the movie somehwere
Kumare - 4/5 Hexaflex Points
Kumare - 4/5 Hexaflex PointsThis is a great documentary film about someone who's fed up with the fake gurus in India, and decides to dress up as a guru and start a mini cult in the US, to prove that anyone can pretend to be a guru and get a cult following.
Has anyone else seen it? I think it's brilliant!
1. Present moment - Kumare does teach people meditation, but it's a fake version, and people start getting the experiencing he's suggesting, so maybe not.
2. Acceptance/Willingness - Interestingly some of his 'followers' full accept him and his 'teachings'. And this shows the danger of gurus.
3. Defusion - Through his teachings, people defuse from their own limiting beliefs, but then they fuse with his beliefs. So this is a great teaching about the danger of fusing from one idea to another.
4. Observer Self - Not touched upon much
5. Values - I'm impressed by the values of the director, to seek the truth
5. Commited Action - The actions of the director/main actor and also how he followed through with what he believed, right through to the end - PS - it's a brilliant ending!
Here's the IMDB link with trailer: https://www.imdb.com/title/tt1865425/
Moonstruck
Moonstruck- Moonstruck
- Fusion (with rules)
- Right from beginning to end, ths movie is so filled with just about every character following rules that clearly are so restrictive on their lives. This makes the movie very funny, enjoyable and accessible, yet incredibly profound. The huge exception to this when the character played by Nicholoas Cage tells a confused woman (Cher) something like "Life is not a storybook, that you can look up to see what to do next. Love is about destroying life ... ..."
- In the context of the movie, these audacious words, just hit out, with an irresistable invitation to vitality - a vivid contrast to following rules blindly (fusion) without any reference to values. The mother with her more philosophical approach would seem to be a contrast to blind rule following, however this is at the cost of avoiding strong emotions (and whatever actions) at her husbands behaviours.
My Life Without Me (2003): 5 hexaflex points
My Life Without Me (2003): 5 hexaflex points- My Life Without Me (2003)
- It’s a beautiful movie of a young woman, Ann. Mother of 2 little kids, living a hard life with little future: low job, husband unemployed, poor housing, little money, little support of her family. One day she discovers that she’s seriously ill and has little time to live. This changes her life and way of life radical. She makes a list of things she wants to do and starts doing them, living life to the max. Very good!
- ACT Principle: Acceptance, Values, Committed Action, Self as context, Mindfulness
SPY KIDS
SPY KIDSI have been using film clips since I was a school counselor and would do in-class interactive social skills lessons. I will bring DVD's into my office and play them for a client on my laptop. One clip I like to use with couples is from the first SPY KIDS film where the mother is telling her kids the story of how she met and married their father. The sequence is beautifully put together in terms of how she and her soon to be husband were spies working on different sides and began dating and hid their connection and then made the commitment. The mother narrates how her commitment to getting married was scarier than any spy mission. The scene of their wedding is a great illustration of commitment and action even in the face of turbulence and threats. Their wedding is interrupted by an attacking helicopter. There is a great shot of the priest holding the Bible while pages are blown out of it by the gusts from the helicopter's blades (challenges to our values and commitment). The last part of the scene that my couples find the most powerful is when the couple is running away and they look into each other's eyes as if telling each other, "I am in this with you no matter what." They then jump off a cliff together and escape into a speeding boat.
Therapeutically, after I show the clip I will invite the client to track in their body to see what was stirred by the images. Film clips are a great way to help clients move from image to sensation and process through fight, flight, and freeze responses.
- Max Stoltenberg, LPC, CHt
Song of the Sea
Song of the SeaIn "Song fo the Sea," this child-friendly movie (https://www.youtube.com/watch?v=HgbXWt8kM5Q) provides really great metaphors for:
(i.) Experiential Avoidance (https://www.youtube.com/watch?v=1mUie8Z85iE);
(ii.) Cost of Avoidance vs. Opening Up (time: ~ 1:01:00 ; https://www.youtube.com/watch?v=IPu4etlfCRg).
It is one of the most beautiful movies I have seen in the past decade!
I hope you find it interesting and/or useful! :)
(Submitted by Jonathan Rhodes on April 19, 2024)
The Shawshank Redemption.
The Shawshank Redemption.The Shawshank Redemption
1.The Shawshank Redemption -pretty much a definitive ACT movie for me! (I recently watched it again within an ACT framework!!)
2. 6 Hexaflex points.
3. As illustrated by:-
CONTACT WITH THE PRESENT MOMENT: Beautifully illustrated in the scene when Andy plays Mozart over the prison and the everybody just stops and listens ( 1 point).
SELF AS CONTEXT: As a punishment for playing the music, Andy is placed into solitary confinement and after his release he tells his fellow convicts that he “had Mr. Mozart to keep me company...[points and taps his head.] It was in here …[gestures over his heart] and in here. That's the beauty of music. They can't get that from you. Haven't you ever felt that way about music?” Red (Morgan Freeman)says that he played the Harmonica as a young man, but lost interest in it and that it didn’t make much sense playing it in prison – Andy says “No, here's where it makes the most sense. You need it so you don't forget”. “Forget?” asks Red, “That there are places in the world that aren't made out of stone. That there's... there's somethin' inside that they can't get to; that they can't touch. It's yours” says Andy (self as context / pure awareness – 1 point).
DEFUSION:Fusion is illustrated when Red says “I’ve been in here most of my life. I’m an institutional man now…just like Brooks was”. Andy replies ““you underestimate yourself” and Red says “I don’t think so” (1 point)
COMMITTED ACTION AND VALUES: Andy talks to Red about his vision of life in a little town in Mexico and life as a free man – he focuses on owning a hotel and a boat (which are goals but I’m sure we could find some values in there somewhere!!) Red (‘passenger on the bus’) says “I don’t think you ought to be doing this to yourself, Andy. I mean mexico is way down there and you’re in here and that’s the way it is”. Andy replies “Yeah right. That’s the way it is. It’s down there and I’m in here. I guess it comes down to a simple choice really…get busy living…or get busy dying”. (highlighting the reality gap between where he is and where he wants to be – within the valued domain of freedom (2 points?)
ACCEPTANCE: Spoiler alert (!) Towards the end of the movie when red is up for parole his rehabilitation officer asks red if he’s been rehabilitated. Red replies “Rehabilitated?... Well, now, let me see. You know, I don't have any idea what that means”. The rehabilitation officer informs Red that it means he is “ready to rejoin society” and Red says “ I know what you think it means, sonny. To me it's just a made-up word. A politician's word, so that young fellas like yourself can wear a suit and a tie and have a job. What do you really wanna know? Am I sorry for what I did? The rehabilitation officer asks “are you?” and Red replies “There's not a day goes by I don't feel regret. Not because I'm in here; or because you think I should. I look back on the way I was then: a young, stupid kid who committed that terrible crime. I want to talk to him. I want to try to talk some sense to him, tell him the way things are. But I can't. That kid's long gone and this old man is all that left. I gotta live with that. Rehabilitated? It's just a bullshit word. So go ahead and stamp your forms, sonny, and stop wasting my time. Because to tell you the truth, I don't give a shit (some acceptance in there!? – 1 point)
MORE COMMITTED ACTION: “ I find I'm so excited I can barely sit still or hold a thought in my head (defusion!) I think it is the excitement only a free man can feel, a free man at the start of a long journey whose conclusion is uncertain I hope I can make it across the border (do what it takes!).. I hope to see my friend (values), and shake his hand. I hope the Pacific is as blue as it has been in my dreams. I hope”
The Zookeeper
The Zookeeper- The Zookeeper - a Ralph Ziman film starring Sam Neill
- Number of Hexaflex points: 3
- A moving film set in an unspecified Eastern European country that has a Bosnian like civil war raging, in which a zookeeper, Ludovic (a superb performance by Sam Neill) is haunted by his past, when he wielded power over a local populace. Only after he meets Ankica ( who, with her son, are refugees from the fighting seeking sanctuary in the now all but deserted zoo) who recounts the horrors she has experienced at the hands of someone in that position, does he begin to accept what he has done, allowing him to emotionally thaw out a little. He also hides his feelings for his dead wife, literally in a box hidden away, which is found by Ankica who tells him his feelings are 'beautiful', again allowing him to accept the caring side of himself (toward people) more. There is an interesting portrayal of the (sometimes) subtle difference between running away from our experience & moving toward a valued direction: Ludovic appears to hold the value of being a good person strongly (represented by him being only one of two people willing to stay on & care for the animals when everyone else has left), but Ankica questions whether this is in fact a cover for running away from connectedness with other people, & by extension, himself. Committed action is demonstrated by Ludovic as he begins his emotional thawing & looks after both Ankica & her son, Zioig, as well as his caring for the zoo animals, & toward the end of the film, himself. This is an interesting portrayal of achieving psychological flexibility: he finally agrees to deviate from his rigid pattern of behaviour (staying with the animals) & leave when it is clear that all is lost. He shows anger initially when this course of action is suggested, much like someone holding on to behaviour that is self-defeating but at least familiar.
- Score: 3/5.
Three Kings (1999) movie
Three Kings (1999) movieThe scene in Three Kings is a post-Desert Storm battle among soldiers.
George Clooney and Spike Jonez are taking cover from the hail of gunfire. Spike's character is afraid of going out and shooting back and the following ensues:
Archie Gates (G.Clooney): You're scared, right?
Conrad Vig (Spike): Maybe.
Archie Gates: The way it works is, you do the thing you're scared shitless of, and you get the courage AFTER you do it, not before you do it.
Conrad Vig: That's a dumbass way to work. It should be the other way around.
Archie Gates: I know. That's the way it works.
- I like this one when talking to 25-39 year old anxious males...Probably not useful for everyone, but I dig it.
Walk The Line
Walk The Line- Walk The Line
- The June Carter character exemplified committed action in the service of a value that was dear to her. The value I would identify (not verbalized by her in the film), would be something like 'Marriage as a committed friendship' or 'Building intimacy'. Some of the elements of committed action on her part included remaining Johnny's friend when he was at his least likeable, rejecting his excessive and self-destructive behaviors while continuing to love him, even remarrying when she couldn't have Johnny. Mind you, he also exemplified similar committed action in continuing to ask her to marry him despite repeatedly being blocked in achieving the desired outcome :).
- ACT Principle: Outcome is the Process through which Process Becomes the Outcome
Yes Man (2008)
Yes Man (2008)- Yes Man (2008)
- The movie is about a man distraught over his girlfriend breaking up with him. He refuses to do anything except stay home and watch videos. His friend drags him to a motivational seminar where the message is "Say YES to Life!" He does and his life changes radically for the better. A very fun romantic comedy with Jim Carrey and Zooey Deschanel.
ACT Relevant Books/Stories
ACT Relevant Books/StoriesChildren's Books for Adults
Children's Books for AdultsOne of my favorite ways to teach defusion is to read children's books to adults, especially books that were likely read to them in childhood like Dr. Seuss and Shel Silverstein, etc. Hearing these stories as an adult helps change their perspective on issues they are facing (I use in a substance use treatment setting, but they can of course be applied to many others). I will start a list of stories that I currently use in my groups, but I'd like to know how many others use this intervention, and what stories you use.
"Oh, The Places You'll Go" by Dr Seuss
"Oh, The Places You'll Go" by Dr SeussPlot from wikipedia
"The story begins with the narrator, relating the decision of the unnamed protagonist (who represents the reader) to leave town. The protagonist travels through several geometrical and polychromatic landscapes and places, eventually encountering a place simply called "The Waiting Place", which is ominously addressed as being a place where everyone is always waiting for something to happen. As the protagonist continues to explore, spurred on by the thoughts of places he will visit and things he will discover, the book cheerfully concludes with an open end."
Hexaflex points addressed
Self-As-Context - At one point the narrator talks about how difficult some of the challenges you will faces will be. "Games you can't win, Cause you'll play against you."
Commited Action - The narrator tells the reader about getting in a slump he states "Unslumping yourself is not easily done." But the point is to keep moving forward
Experiential Avoidance - The Waiting Place is where people are waiting for things to happen to them instead making things happen. It doesn't say exactly why, but I think it's fair to say that they are waiting to avoid being uncomfortable. This reminds me of the Waiting for the Wrong Train metaphor.
"The Giving Tree" by Shel Silverstein
"The Giving Tree" by Shel SilversteinI think that this book was written to show how far a parent would go for their child. When I read it though, I leave out the last couple pages, because I use this story a lot to show the impact of codependence on anything (substances for my treatment). The tree represents the patient, and the boy represents drugs. Sometimes I pull in some RFT principles and have the patients imagine what the experience is like for the apples, or the leaves, or the boat.
Plot from Wikipedia
The book follows the lives of a female apple tree and a boy, who develop a relationship with one another. The tree is very "giving" and the boy evolves into a "taking" teenager, man, then elderly man. Despite the fact that the boy ages in the story, the tree addresses the boy as "Boy" his entire life.
In his childhood, the boy enjoys playing with the tree, climbing her trunk, swinging from her branches, carving "Me + T (Tree)" into the bark, and eating her apples. However, as the boy grows older, he spends less time with the tree and tends to visit her only when he wants material items at various stages of his life, or not coming to the tree alone (such as bringing a lady friend to the tree and carving "Me +Y.L." (her initials) into the tree. In an effort to make the boy happy at each of these stages, the tree gives him parts of herself, which he can transform into material items, such as money (from her apples), a house (from her branches), and a boat (from her trunk). With every stage of giving, "the Tree was happy".
In the final pages, both the tree and the boy feel the sting of their respective "giving" and "taking" nature. When only a stump remains for the tree (including the carving "Me + T"), she is not happy, at least at that moment. The boy does return as a tired elderly man to meet the tree once more. She tells him she is sad because she cannot provide him shade, apples, or any materials like in the past. He ignores this and states that all he wants is "a quiet place to sit and rest," which the tree, who is weak being just a stump, could provide. With this final stage of giving, "the Tree was happy".
Hexafles processes addressed
Fusion - The Tree fuses to the thought that it can only be happy when The Boy was around or when she doing something for The Boy. It even becomes literally fused to when intitials are carved into The Tree.
Experiential Avoidance - The Tree will do anything she can to avoid making The Boy feel like he can't do anything, because that would make her sad.
When sadness is at your door
When sadness is at your doorChinese Farmer Story
Chinese Farmer StoryI heard this story in passing years ago, and have used iterations of it. It was only after learning more about ACT had I realized I was using a story to relate avoiding fusion to thoughts positive or negative thoughts/feelings. This iteration I borrowed online, but provide the name of the source:
The Story of the Chinese Farmer
Once upon a time there was a Chinese farmer whose horse ran away. That evening, all of his neighbors came around to commiserate. They said, “We are so sorry to hear your horse has run away. This is most unfortunate.” The farmer said, “Maybe.” The next day the horse came back bringing seven wild horses with it, and in the evening everybody came back and said, “Oh, isn’t that lucky. What a great turn of events. You now have eight horses!” The farmer again said, “Maybe.”
The following day his son tried to break one of the horses, and while riding it, he was thrown and broke his leg. The neighbors then said, “Oh dear, that’s too bad,” and the farmer responded, “Maybe.” The next day the conscription officers came around to conscript people into the army, and they rejected his son because he had a broken leg. Again all the neighbors came around and said, “Isn’t that great!” Again, he said, “Maybe.”
The whole process of nature is an integrated process of immense complexity, and it’s really impossible to tell whether anything that happens in it is good or bad — because you never know what will be the consequence of the misfortune; or, you never know what will be the consequences of good fortune.
Alan Watts
Enchiridion of Epictetus
Enchiridion of EpictetusThis is my paraphrase of the famous brief Stoic work, with the sections labeled with the Core Flexibility Processes - because they just seem to fit so well. This might be a source of new stories or metaphors for your work. Epictetus doesn't always sound like an ACT therapist - but almost always.
Perhaps
PerhapsThe Little Prince
The Little PrinceFrom The Little Prince by Antoine de Saint-Exupery
This is from one of my favourite books.
It has many ACT relevant moments in it, this is just one of them:
The next planet was inhabited by a tippler. This was a very short visit, but it plunged the little prince into deep dejection.
"What are you doing there?" he said to the tippler, whom he found settled down in silence before a collection of empty bottles and also a collection of full bottles.
"I am drinking," replied the tippler, with a lugubrious air.
"Why are you drinking?" demanded the little prince.
"So that I may forget," replied the tippler.
"Forget what?" inquired the little prince, who already was sorry for him.
"Forget that I am ashamed," the tippler confessed, hanging his head.
"Ashamed of what?" insisted the little prince, who wanted to help him.
"Ashamed of drinking!" The tippler brought his speech to an end, and shut himself up in an impregnable silence.
And the little prince went away, puzzled. "grown-ups are certainly very, very odd," he said to himself, as he continued on his journey.
I think this makes some nice ACT-relevant points about fusion, experiential avoidance and the futility of avoidance/control strategies.
The tippler is fused with his feeling of shame to the extent that he must avoid it by drinking. However, the costs and consequences of his drinking is further shame that he also fuses with and must avoid, also by drinking.
The tippler is essentially drowning in an alcoholic quicksand. The more he drinks to escape, the more bad stuff shows up, so the more he has to drink to escape a little bit more.
The Little Prince, who is essentially a child who has lived alone and has not been exposed to a verbal community where fusion and avoidance repertoires have fully developed sees this as being very odd indeed.
Things the grandchildren should know
Things the grandchildren should knowFor a great example of someone dignifying their values with pain, I can whole-heartedly recommend the autobiography "Things the grandchildren should know" by Mark Everett (Lead singer of the band Eels). http://en.wikipedia.org/wiki/Things_the_Grandchildren_Should_Know
From publisher:
How does one young man survive the deaths of his entire family and manage to make something of his life? The insecure son of a misunderstood genius of quantum mechanics, Mark Oliver Everett's upbringing was "ridiculous, sometimes tragic, and always unsteady." But somehow he survived this and ensuing tragedies, channeling his experiences into his critically acclaimed music with the Eels.
Told with surprising candor, his memoir is an inspiring and remarkable story, full of hope, humor, and wry wisdom.
ACT Relevant Songs
ACT Relevant Songs
Sometimes it can be useful to play a piece of music at the beginning of a session or a group to more rapidly create a particular emotional tone for doing a certain piece of work in ACT.
If you use any music with clients, workshops, or groups, please share below so that others can benefit.
For example, I know that John Forsyth said that sometimes he uses Johnny Cash's cover of "Hurt" as an opening for his workshops.
To contribute your song, click on "add child page" below.
In the Body section of the Edit page, type
- My song
- ACT Principle: Defusion (or whatever it is)
- Any recommendations on how to use the song
Hint: You can copy and paste the text above so that you don't have to keep track of all the HTML code.
Looking forward to the ideas. Cheers!
Acceptance and Commitment Song - Lou Lasprugato
Acceptance and Commitment Song - Lou LasprugatoAcceptance and Commitment Song - Lou Lasprugato
Lyrics:
There's suffering when you run away from pain
Expecting change but doing more of the same
And it's a long way down when your mind pushes you around
Open up
Open up
Step into this space
See what you need to face
To get through
To get through
What matters to you
What matters to you
It's hard when love's all but lost
And your best is not good enough
And you fill with fear when you're anywhere but here
Open up
Open up
Step into this space
See what you need to face
To get through
To get through
What matters to you
What matters to you
As you move
As you sway
In the eye of the storm
In the depths of the pain
Will you take a stand?
Will you carry me?
Will you notice hurt?
Will you let it be?
Will you take a stand?
Will you carry me?
Will you notice love?
Will you let it be?
And breathe...
Amos Lee - Supply and Demand
Amos Lee - Supply and DemandACT Principle: Creative Hopelessness and missing out on Values
Any recommendations on how to use the song : A fellow ACT therapist used hits during one of the first sessions of an Anger group.
Here's the lyrics:
Somethin’ gotta give with the way I’m livin’
Seems I’m gettin’ down everyday
The more I strive, the less I’m alive
And seems i’m gettin’ further away
Oh well all my superstitions and my crazy suspicions
Of the people that I care about
I been doin’ more screamin’ than i been doin’ dreamin’
And I think it’s time I figured it out
Yeah baby I need a plan to understand
That life ain’t only supply and demand
I been goin’ joggin’ in the park after dark
Draggin’ ’round with me my ball and chain
Took southern skies to make me realize
That I’m causin’ myself this pain
The woman that I’m lovin’ yeah I’m pushin’ and shovin’
Getting further on by the day
And I can’t understand how the heart of this man
Ever let it end up this way
Yeah baby I need a plan to understand
That life ain’t only supply and demand
When the road gest dark and lonesome dear
You can find me here
But honey you don’t know where I am
You need a friieend yeeaahh
Life ain’t easy in fact I know it’s sleazy
When you’re the big man in town
Shakin’ religions and makin’ decisions
You never get slow on down
Well your wife and your baby you tell them yeah well maybe
I’ll meet y’all at a weekend resort
Put your eyes on the prize and you can realize
Your little girl’s life’s so short
Brother you need a plan to understand
That life ain’t only supply and demand
Yeah sister you need a plan to understand
That life ain’t only supply and demand
Hey, you better figure it out now
You know you ain’t comin’ back down, yeah
You better figure it out now
You know you ain’t comin’ back down
Submitted by Catherine B. Clemmer, MSW, LCSW
Cat Stevens - if you want to sing out
Cat Stevens - if you want to sing outCommited action, Values
If You Want to Sing Out, Sing Out Songtext
Well, if you want to sing out, sing out
and if you want to be free, be free
'cause there's a miilion things to be
you know that there are.
And if you want to live high, live high
and if you want to live low, live low
'cause there's a million ways to go
you now that there are.
You can do what you want
the opportunity's on
and if you find a new way
you can do it today
you will make it all true
and you can make it undo
you see ah ah, it's easy ah ah,
you only need to know.
Well, if you want to say yes, say yes
and if you want to say no, say no
'cause there's a million ways to go
you know that there are
Ansd if you want to be me, be me
and if you want to be you, be you
'cause there's a million things to do
you know that there are.
You can do what you want
the opportunity's on
and if you find a new way
you can do it today
you will make it all true
and you can make it undo
you see ah ah, it's easy ah ah,
you only need to know.
Well, if you want to sing out, sing out
and if you want to be free, be free
'cause there' s a million things to be
you know that there are
you know that there are
you know that there are
you know that there are.
Colin Hay - Overkill
Colin Hay - OverkillOriginally submitted by Nick Frye
I think this song is such as great description of cognitive fusion and could be used to help explain that concept as well as using the lyrics "ghosts appear then fade away" as a great to discuss defusion.
"Overkill"
I can't get to sleep
I think about the implications
Of diving in too deep
And possibly the complications
Especially at night
I worry over situations
I know we'll be alright
Perhaps it's just imagination
Day after day it reappears
Night after night my heartbeat shows the fear
Ghosts appear and fade away
Come back another day
Alone between the sheets
Only brings exasperation
It's time to walk the streets
Smell the desperation
At least there's pretty lights
And though there's little variation
It nullifies the night from overkill
Day after day it reappears
Night after night my heartbeat shows the fear
Ghosts appear and fade away
Come back another day
I can't get to sleep
I think about the implications
Of diving in too deep
And possibly the complications
Especially at night
I worry over situations that
I know will be alright
It's just overkill
Day after day it reappears
Night after night my heartbeat shows the fear
Ghosts appear and fade away
Ghosts appear and fade away
Ghosts appear and fade away
Drive--Incubus
Drive--IncubusHi,
Great idea!
I haven't used this with clients, but I've always thought the song "Drive" by Incubus is very ACT consistent.
Here's the first verse: "Sometimes, I feel the fear of uncertainty stinging clear And I can't help but ask myself how much I'll let the fear take the wheel and steer. It's driven me before, and it seems to have a vague, haunting mass appeal. But lately I'm beginning to find that I should be the one behind the wheel."
Could be used in conjunction with the monsters-on-the-bus exercise, or any number of exercises that focus on avoidance.
Mary
Gossip - Move in the right direction
Gossip - Move in the right directionAcceptance and commited action (*there is just one unfortunate limitation in the song, which is the sentence "I hold back tears" - it is not ACT-conform)
Move in the Right Direction
Gossip
One step closer, I'm feeling fine
Getting better one day at a time
I'm moving forward with all of my might
I'm headed toward a new state of mind
So I hold back tears*
Move in the right direction
Face my fears
Move in the right direction
I'm doing fine
One step closer every day at a time
I won't lose my mind, lose my mind
Uh-uh... oooooh
Motivation of powerful strength
Hesitation was my first instinct
I got the notion my weakness was
Total devotion, it's okay because
I will hold back tears*
So I can move in the right direction
I have faced my fears
Now I can move in the right direction
I'm doing fine
One step closer every day at a time
I won't lose my mind, lose my mind
Uh-uh... oooooh
Keeping my head up
Looking forward
Reminiscing will get you nowhere
Never say never
Starting over
It's not perfect, but it's getting closer
I'll hold back tears*
So I can move in the right direction
I have faced my fears
Now I can move in the right direction
I'm doing fine
One step closer every day at a time
I won't lose my mind, lose my mind
Uh-uh... oooooh
Keep Breathing By Ingrid Michaelson
Keep Breathing By Ingrid MichaelsonThis song is about being in the present moment and recognizing what you have control over and what you don't have control over. It is also about not being "hooked" by your thoughts.
L.A. Song by Beth Hart
L.A. Song by Beth HartThis song is great at illustrating how a woman was using emotional avoidance to escape from emotional pain. She eventually realizes that she needs to face her emotions and her issues directly she needs to come towards them rather than run from them. She chooses to engage in committed action by returning to L.A. After she has this realization, her emotional pain subsides.
Life is Hard - Edward Sharpe and the Magnetic Zeroes
Life is Hard - Edward Sharpe and the Magnetic Zeroesa great song about acceptance (and of course because its sung, it is defusion as well)
"Life Is Hard"
Life is beauty through and through
Life is sunny, life is cool
Life is even easy too
But if my word is to be true
Life is something to behold
But if the truth is to be told
Let us not leave out any part
Do not fear, it's safe to say it here
You will not be called a weakling nor a fraud
For feeling the pain of the whole wide world
You want to help but can't help the feeling you cannot
And it's killing you while you're just trying to smile from your heart
So go on, say it, on the same knees you're praying
Yes, life is hard
Come celebrate
Life is hard
Come celebrate Life is hard
Our life is all we are
Celebrate it in the sun, promenade it with everyone
Elevate it in a song
And I'll be there to play it, don't get me wrong
When I feel like dying and being gone
When life is hard
There's just one thing, let's not forget
Yes! life is it!
Life is it, life is it, it's where it's at
It's getting skinny, getting fat
It's falling deep into a love,
It's getting crushed just like a bug
Life there's no love, it's getting beat into the ground
It's getting lost and getting found,
To growing up and getting round
It's feeling silence, feeling sound
It's feeling lonely, feeling full
It's feeling oh so beautiful!
Yes!
Come celebrate
Life is hard
Come celebrate
Life is hard
Our life is all we are
Linkin Park - Heavy
Linkin Park - HeavyThis song demonstrates the concepts of Acceptance, Being Present, Defusion, and Self As Context
I don't like my mind right now
Stacking up problems that are so unnecessary
Wish that I could slow things down
I wanna let go but there's comfort in the panic
And I drive myself crazy
Thinking everything's about me
Yeah, I drive myself crazy
'Cause I can’t escape the gravity
I'm holding on
Why is everything so heavy?
Holding on
So much more than I can carry
I keep dragging around what's bringing me down
If I just let go, I'd be set free
Holding on
Why is everything so heavy?
You say that I'm paranoid
But I'm pretty sure the world is out to get me
It's not like I make the choice
To let my mind stay so fucking messy
I know I'm not the center of the universe
But you keep spinning 'round me just the same
I know I'm not the center of the universe
But you keep spinning 'round me just the same
I'm holding on
Why is everything so heavy?
Holding on
So much more than I can carry
I keep dragging around what's bringing me down
If I just let go, I'd be set free
Holding on
Why is everything so heavy?
I know I'm not the center of the universe
But you keep spinning 'round me just the same
I know I'm not the center of the universe
But you keep spinning 'round me just the same
And I drive myself crazy
Thinking everything’s about me
Holding on
Why is everything so heavy?
Holding on
So much more than I can carry
I keep dragging around what's bringing me down
If I just let go, I'd be set free
Holding on
Why is everything so heavy?
Why is everything so heavy?
Why is everything so heavy?
Live Like A Warrior
Live Like A WarriorGood song for diffusion - especially if you sing it :)
https://www.youtube.com/watch?v=p53pDNodxHE
Live Like You Were Dying--Tim McGraw
Live Like You Were Dying--Tim McGrawSong: Live Like You were Dying--Tim McGraw
ACT concepts: Mindfulness/Awareness:
"...and I watched an eagle as it was flying"
Values:
"and I loved deeper
and I spoke sweeter
and I gave forgiveness I'd been denying
and he said someday I hope you get the chance
to live like you were dying
He said I was finally the husband
that most the time I wasn't
and I became a friend
a friend would like to have
and all the sudden going fishin
wasn't such an imposition
and I went three times
that year I lost my dad"
Again, not sure how to use this in therapy, but pretty ACT consistent.
Mixtapes - Bad Parts
Mixtapes - Bad PartsACT Principle(s): Acceptance, Committed Action
Recommendations On Use: I have not used this song clinically yet. I'm a trainee, and have hesitated based on (1) the blatant (though effective) use of a top 7 swear word, and (2) the VERY pop-punk sound, which I happen to love, but recognize many people find grating. That being said, as a clinician working with young adults with SUDs in various stages of readiness to change their substance use, it feels particularly fitting. I may bring it to a second-year practicum in my role as an advanced student supervisor first.
Lyrics:
I don't know what we're doing this for
Say we're getting better while we're passed out on the floor
And then we find a way to forget through the years
We wish the bad parts would just disappear
But they're not going anywhere
We're not going any-
Where
I wish I could tell you why I
Have this need to get the hell out before I die.
I'm not kidding myself that it's different somewhere else
Guess I just want to try and find new faces who don't want to just forget
Instead of lubing up the awkward parts
They want to break their fucking habits.
It's time
We stop saying why
And make it fucking happen
And make something happen
No, no
Hannah told me she's unhappy all the time she's been in school
But she does it anyway
Hey, Christina does it too
And Sarah told me her relationship was making her blue
But she takes what she can get
And when she can forget
The things he called her last night
She knows he's heaven-sent.
It's time
We stop saying why
And make it fucking happen
And make something happen
No, no
Nickelback- If today was your last day
Nickelback- If today was your last dayNickelback- If today was your last day https://www.youtube.com/watch?v=BtlsyifVaMI
My best friend gave me the best advice
He said each day's a gift and not a given right
Leave no stone unturned, leave your fears behind
And try to take the path less traveled by
That first step you take is the longest stride
If today was your last day
And tomorrow was too late
Could you say goodbye to yesterday?
Would you live each moment like your last?
Leave old pictures in the past
Donate every dime you have?
If today was your last day
(If today was your last day)
Against the grain should be a way of life
What's worth the prize is always worth the fight
Every second counts 'cause there's no second try
So live like you'll never live it twice
Don't take the free ride in your own life
If today was your last day
And tomorrow was too late
Could you say goodbye to yesterday?
Would you live each moment like your last?
Leave old pictures in the past
Donate every dime you have?
Would you call old friends you never see?
Reminisce old memories
Would you forgive your enemies?
Would you find that one you're dreamin' of?
Swear up and down to God above
That you finally fall in love
If today was your last day
If today was your last day
Would you make your mark by mending a broken heart?
You know it's never too late to shoot for the stars
Regardless of who you are
So do whatever it takes
Cause you can't rewind a moment in this life
Let nothin' stand in your way
Cause the hands of time are never on your side
If today was your last day
And tomorrow was too late
Could you say goodbye to yesterday?
Would you live each moment like your last?
Leave old pictures in the past
Donate every dime you have?
Would you call old friends you never see?
Reminisce old memories
Would you forgive your enemies?
Would you find that one you're dreamin' of?
Swear up and down to God above
That you finally fall in love
If today was your last day
Sarah Blasko - Always on this line
Sarah Blasko - Always on this lineFusion; the song (and the video) illustrates rigid rule-governed behavior and its costs, like the lack of and longing for vitality.
Always on this line
As the day turns to night
under these suburban skies
think of all willing lies, of cutting ties,
the emptiness,
At first light, first sight,
the world seems like a miracle,
but try to hold it in your hands
and watch it get away,
oh the ugliness of fate,
When you're always on this line,
when you're always on this line,
you could've crossed a million times,
but you're always on this line,
oh, put your hands up,
claim your crime,
'cause you never had the time,
you still get to work just fine,
when you're always on this line
But it's alright, it's okay,
when there's excuses in your way,
you can try, just make it up,
settle down but don't look up,
At first bite, first lie,
the world seems like it serves you well,
but try to catch it in your hands,
treating it like a slave of the emptiness you crave,
When you're always on this line,
when you're always on this line,
you could've crossed a million times,
but you're always on this line,
oh, put your hands up,
claim your crime,
'cause you never had the time,
you still get to work just fine,
when you're always on this line,
Oh, it might be unkind of me to make you feel bad,
it might be a shame of me to treat you like that,
when there's everything you've worked for in your life,
on this line,
When you're always on this line,
when you're always on this line,
you could've crossed a million times,
but you're always on this line,
oh, put your hands up,
claim your crime,
'cause you never had the time,
you still get to work just fine,
when you're always on this line
The Art of Letting Go - Rachel Collis
The Art of Letting Go - Rachel CollisIt's beautiful and the lyrics are very ACT consistent.
The Competition - Kimya Dawson
The Competition - Kimya DawsonThe Competition - Kimya Dawson
ACT Principle: Acceptance This song is great for helping people grasp the concepts of acceptance and willingness in the midst of strong emotions and unhelpful thoughts. Popular with adolescents and younger generation clients (especially those who have seen the film Juno and may be familiar with other songs by Kimya Dawson).
The Hellacopters - Monkeyboy
The Hellacopters - Monkeyboya song that problematizes fusion and thereby creates defusion :)
Monkeyboy - The Hellacopters
I got an ape performing in my head
If he don't stop then I will soon be dead
This monkey's no friend of mine
I try to act straight but he's on cloud number nine
He's got a cup made of tin
And it's 'cause of him you won't let me in
He bangs a drum so I can't get no sleep
Well he's a monkey but he can't be beat
Head over heels on banana peel
I'm getting confused as to what I feel
And every time I try to speak
He always puts his monkeytongue in my cheek
Oh, my, my - I'd do anything to make him die
And oh then I'd see there's nothing I can do
The monkey's just a part of me
I got a monkey singing in my brain
I should have known already we're the same
Oh, my, my - I'd do anything to make him die
And oh then I'd see there's nothing I can do
The monkey's just a part of me
The Trouble with Humans
The Trouble with HumansTurn It Off (The Book of Mormon)
Turn It Off (The Book of Mormon)Originally submitted by Deborah Stringer
The song "turn it off" from the musical "book of mormon" is a satirical tap number about the unworkability of the control agenda. It was written by the same folks who do South Park, so, as you might expect, it's not for all clients or clinicians. The lyrics are below:
The Book of Mormon lyrics: Turn it Off
I got a feeling that you could be feeling
A whole lot better than you feel today
You say you got a problem, well that's no problem
It's super easy not to feel that way
When you start to get confused because of thoughts in your head
Don't feel those feelings hold them in instead
Turn it off, like a light switch
Just go click
It's a cool little Mormon trick
We do it all the time
When you're feeling certain feelings
That just don't seem right
Treat those pesky feelings like a reading light
And turn em off like a light switch
Just go bap
Really what's so hard about that?
Turn it off
Turn it off
When I was young my dad would treat my mom real bad
Every time the Utah Jazz would lose
He'd start a-drinking and I'd start a-thinking
How am I gonna keep my mom from getting abused
I'd see her all scared and my soul was dyin'
My dad would say to me now don't you dare start cryin'
Turn it off
Like a light switch
Just go flick
It's our nifty little Mormon trick
Turn it off
Turn it off
My sister was a dancer but she got cancer
The doctor said she still had two months more
I thought she had time so I got in line
For the new iPhone at the apple store
She laid there dying with my father and mother
Her very last words were where is my brother
Turn it off
Bid those sad feelings adieu
The fear that I might get cancer too
When I was in fifth grade I had a friend Steve Blade
He and I were close as two friends could be
One thing led to another and soon I would discover
I was having really strange feelings for Steve
I thought about us on a deserted island
We'd swim naked in the sea and then he'd try and...
Whoa!
Turn it off like a light switch
There it's gone (good for you!)
My hetero side just won
I'm all better now
Boys should be with girls that's heavenly father's plan
So if you ever feel you'd rather be with a man
Turn it off
Well, Elder McKinley, I think it's okay that you're having gay thoughts
Just so long as you never act upon them
No – cause then you're just keeping it down
Like a dimmer switch
On low (on low)
Thinking nobody needs to know (uh oh)
But that's not true
Being gay is bad but lying is worse
So just realize you have a curable curse
And turn it off
Turn it off
(Tap dancing! With red sparkly vests!)
Turn it off
Now how do you feel?
The same (ahw)
Then you've only got yourself to blame
You didn't pretend hard enough
Imagine that your brain is made of tiny boxes
Then find the box that's gay and crush it!
Okay?
No, no I'm not having gay thoughts
Alright! It worked! Yay!
Turn it off
Turn it off, turn it off
Turn it off, turn it off like a light switch
Just go click (click, click)
What a cool little Mormon trick (trick, trick)
We do it all the time
When you're feeling certain feelings that just don't seem right (don't seem right)
Treat those pesky feelings like a reading light
Turn it off like a light switch on a cord
Now he isn't gay any...
Turn it, turn it, turn it, turn it
Turn it, turn it, turn it, turn it
Turn it
Turn it off (off!)
Two ACT consistent Eels songs.
Two ACT consistent Eels songs.For a great example of someone dignifying their values with pain, I can whole-heartedly recommend the autobiography "Things the grandchildren should know" by Mark Everett (Lead singer Eels).
http://en.wikipedia.org/wiki/Things_the_Grandchildren_Should_Know
His songs also hint at vital living: -----------------------------------------------------
Hey Man (Now You're Really Living):
Do you know what it's like to fall on the floor?
Cry your guts out till you got no more
Hey man, now you're really living
Have you ever made love to a beautiful girl?
Made you feel like it's not such a bad world
Hey man, now you're really living
Now you're really giving everything
And you're really gettin' what you gave
Now you're really livin' what this life is all about
Well, I just saw the sun rise over the hill
Never used to give me much of a thrill
But, hey man, now I'm really living
Do you know what it's like to care too much?
About someone that you're never gonna get to touch
Hey man, now you're really living
Have you ever sat down in the fresh-cut grass
And thought about the moment and when it will pass
Hey man, now you're really living
Now you're really giving everything
And you're really gettin' what you gave
Now you're really livin' what this life is all about
Now, what would you say if I told you that
Everyone thinks you're a crazy old cat
Hey man, now you're really living
Do you know what it's like to fall on the floor?
Cry your guts out till you got no more
Hey man, now you're really living
Have you ever made love to a beautiful girl?
Made you feel like it's not such a bad world
Hey man, now you're really living...
----------------------------------------------
P.S. You rock my world:
I was at a funeral the day i realized
I wanted to spend my life with you
Sitting down on the steps at the old post office
The flag was flying at half-mast
And I was thinkin' 'bout how everyone is dying
And maybe it's time to live
I don't know where we're going
I don't know what we'll do
Walked into the thrif-tee
Saw the man with the hollow eyes
who didn't give me all my change
But it didn't bother me this time
'cause I know I've only got this moment
And it's good
I went to the gas station
Old woman honked her horn
Waiting for me to fix her car
I don't know where we're going
I don't know what we'll do
Laying in bed tonight
I was thinking and listening to
all the dogs and the sirens and the shots
And how a careful man tries to dodge the bullets
While a happy man takes a walk
And maybe it's time to live ----------------------------------------------------
Various ACT Related Song Lyrics
Various ACT Related Song Lyrics18 Song lyrics that cover a broad range of ACT concepts...Here are some ACT themes covered by various songs. See the attached file for the actual lyrics (note, some of them are abridged):
Suffering is Universal:
R.E.M. - Everybody Hurts
TOAD THE WET SPROCKET - Little Buddha
The Problem:
RADIOHEAD - Fitter Happier
NADA SURF - Stalemate
SUPREME BEINGS OF LEISURE - What's the Deal
Acceptance:
THE BEATLES - Let it Be
JAMES BROWN - Mind Power
NITIN SAWHNEY - Letting Go
Mindfulness:
MEREDITH MONK - Walking Song (no lyrics, just breathing)
Self as Context:
AKRON/FAMILY - Franny/You're Human
NINE INCH NAILS - Only T.REX - Cosmic Dancer
Values:
ECHO AND THE BUNNYMEN - What are you Going to do with Your Life?
LIONEL RITCHIE - Time
TIM MCGRAW - Live Life Like You were Dying
Willingness:
DURAN DURAN - Finest Hour
SLY AND THE FAMILY STONE - Stand!
FRANK SINATRA - My Way
Walk Unafraid - First Aid Kit/ REM
Walk Unafraid - First Aid Kit/ REMThis song is called Walk Unafraid, it was originally made by R.E.M and then covered by First Aid Kit for the recent move Wild. I like this because it's about encouraging someone to be willing to make a change, sitting with (or carrying) negative emotion or pain. This is especially in the lines
'If I have a bag of rocks to carry as I go
I just want to hold my head up high
I don't care what I have to step over'
As I see it, this song is about willingness to walk unafraid even in the presence of fear and doubt. The person may be clumsy and fall and trip but she will pick herself up and carry on. Expanding the opportunities open to her and holding her head high.
As the sun comes up, as the moon goes down
These heavy notions creep around
It makes me think, long ago
I was brought into this life, a little lamb
A little lamb
Courageous, stumbling
Fearless was my middle name
But somewhere there I lost my way
Everyone walks the same
Expecting me to step
The narrow path they've laid
They claim to
[Chorus]
Walk unafraid
I'll be clumsy instead
Hold me love or leave me high
[Verse 2]
Say "keep within the boundaries if you want to play"
Say "contradiction only makes it harder"
How can I be
What I want to be
When all I want to do is strip away
These stilled constraints
And crush this charade
Shred this sad masquerade
I don't need no persuading
I'll trip, fall, pick myself up and
[Chorus]
Walk unafraid
I'll be clumsy instead
Hold me love or leave me high
[Verse 3]
If I have a bag of rocks to carry as I go
I just want to hold my head up high
I don't care what I have to step over
I'm prepared to look you in the eye
Look me in the eye
And if you see familiarity
Then celebrate the contradiction
Help me when I fall to
[Chorus]
Walk unafraid
I'll be clumsy instead
Hold me love or leave me high
[Chorus]
I will walk unafraid
I'll be clumsy instead
Hold me love or leave me high
[Outro]
Hey, hey, hey, hey, hey, hey
Hey, hey, hey, hey, hey, hey
Hey, hey, hey, hey, hey, hey
Hey, hey, hey, hey, hey, hey
ACT relevant poems
ACT relevant poemsACT POEMS
A key feature of clinical ACT work is the de-literalization of language and cognition. Metaphor, story, experiential exercises, art work and other techniques can facilitate this perspective shift for clinicians and clients alike. Although poetry uses the medium of language, the art and magic of poetry is often written from and can be received by the spaciousness of the self as context.
These poems can be used in clinical settings to illustrate, inspire and motivate around the six core processes of ACT.
“Poetry connects us to what is deepest in ourselves. It gives us access to our own feelings, which are often shadowy, and engages us in the art of making meaning. It widens the space of our inner lives. It is a magical, mysterious, inexplicable (though not incomprehensible) event in language.” Quote from Edward Hirsch.
“Life is neither meaningful nor meaningless. Meaning and its absence are given to life by language and imagination. We are linguistic beings who inhabit a reality in which it makes sense to make sense. For life to make sense it needs purpose. Even if our aim in life is to be totally in the here and now, free from past conditioning and any idea of a goal to be reached, we still have a clear purpose – without which life would be meaningless. A purpose is formed of words and images. And we can no more step out of language and imagination than we can step out of our bodies.” Stephen Bachelor - Buddhism without Beliefs
I've also attached the poster I did for Parma World Con and these same poems in word format. Enjoy :-)
ACT Poems
The Serenity Prayer
Grant me the serenity to
Accept the things I cannot change;
Courage to change the things I can; and
Wisdom to know the difference
DEFUSION
The Guest House-- Jelaluddin Rumi, translation by Coleman Barks
This being human is a guest house.
Every morning a new arrival.
A joy, a depression, a meanness,
some momentary awareness comes
as an unexpected visitor.
Welcome and entertain them all!
Even if they are a crowd of sorrows,
who violently sweep your house
empty of its furniture,
still, treat each guest honourably.
He may be clearing you out
for some new delight.
The dark thought, the shame, the malice.
meet them at the door laughing and invite them in.
Be grateful for whatever comes.
because each has been sent
as a guide from beyond.
Also From Rumi
Out beyond our ideas
Of wrong doing
And right doing
There is a field.
I’ll meet you there.
When the soul lies down in that grass
The world is too full to talk about.
Ideas, language, even the words
You and me
Have no meaning.
INSIDE by NeLi Martin
I don’t work for the CIA
MI5 or the FBI,
But I have a secret life
Inside.
While they talk and share –
Try to connect,
I’m running a different show,
It’s like multi-plex.
ACCEPTANCE
Kindness – Namoi Shihab Nye
Before you know what kindness really is
you must lose things,
feel the future dissolve in a moment
like salt in a weakened broth.
What you held in your hand,
what you counted and carefully saved,
all this must go so you know
how desolate the landscape can be
between the regions of kindness.
How you ride and ride
thinking the bus will never stop,
the passengers eating maize and chicken
will stare out the window forever.
Before you learn the tender gravity of kindness,
you must travel where the Indian in a white poncho
lies dead by the side of the road.
You must see how this could be you,
how he too was someone
who journeyed through the night with plans
and the simple breath that kept him alive.
Before you know kindness as the deepest thing inside,
you must know sorrow as the other deepest thing.
You must wake up with sorrow.
You must speak to it till your voice
catches the thread of all sorrows
and you see the size of the cloth.
Then it is only kindness that makes sense anymore,
only kindness that ties your shoes
and sends you out into the day to mail letters and
purchase bread,
only kindness that raises its head
from the crowd of the world to say
it is I you have been looking for,
and then goes with you everywhere
like a shadow or a friend.
St. Francis And The Sow by Galway Kinnell
The bud
stands for all things,
even those things that don't flower,
for everything flowers, from within, of self-blessing;
though sometimes it is necessary
to reteach a thing its loveliness,
to put a hand on its brow
of the flower
and retell it in words and in touch
it is lovely
until it flowers again from within, of self-blessing;
as St. Francis
put his hand on the creased forehead
of the sow, and told her in words and in touch
blessings of earth on the sow, and the sow
began remembering all down her thick length,
from the earthen snout all the way
through the fodder and slops to the spiritual curl of
the tail,
from the hard spininess spiked out from the spine
down through the great broken heart
to the blue milken dreaminess spurting and shuddering
from the fourteen teats into the fourteen mouths sucking
and blowing beneath them:
the long, perfect loveliness of sow.
INTREPID ADVENTURER by NeLi Martin
Intrepid adventurer
– Soft with determination
– Brave and courageous.
Many lands and landscapes traversed
Many encounters
In the quest for Freedom,
Truth,
Love.
Meanwhile
Loneliness, cold with despair, lies coiled.
Huddled into itself.
Asleep.
Shame hatred and unworthiness – all
Keep me from seeing
The task is also
To be willing to be found.
Gratitude
Humility
Gladness…
I find I am found
Joy
STEEL WOOLY THOUGHTS - NeLi Martin April 2005
The harshness of confusion
Scratches and tears at the flesh –
Wounds deepen
As I flail in pitiful attempts
At understanding.
Not realising
Freedom lies
Patiently awaiting my surrender.
LET THE WOUND LIE OPEN by Michael Leuni, Common Prayer Collection
When the heart
Is cut or cracked or broken
Do not clutch it
Let the wound lie open
Let the wind
From the good old sea blow in
To bathe the wound with salt
and let it sting
Let a stray dog lick it.
Let a bird lean in the hole and sing,
A simple song like a tiny bell
And let it ring
Let it go. Let it out.
Let it all unravel.
Let it free and it can be
A path on which to travel.
ANGER by NeLi Martin
Angry bitter in my teeth
Angry acid on my tongue
- How could you?
- Why would you?
Vengeance will be ……. Whose?
Nothing sweet
Here, is my life
Bound and battered by
Outrage and
Righteous
Indignation
And you just want to see my churlish
Girlish
Femme fatale.
But this bubbling cauldron of rage
This endless fury
Cannot, And never will
release me
Into the world.
Fair of Face and Full of Grace (Not) – NeLi Martin
The cards are dealt.
They flutter through the air
So full of possibility;
Innocent.
Anticipation …..
Gives way to expectation.
However, what is revealed
In the stark light
Of everyday life
Seems to deflate.
Let down.
In comparison to some
Just not fair.
BUT IT’S NOT FAIR
IT’S JUST NOT FAIR!
This is not the life I dreamed.
You don’t understand…
There was that promise –
That I would be special.
My life was supposed to mean
Something
To someone.
It’s not fair!
You don’t understand.
Misunderstood.
Miserably misunderstood
Misery.
Stuck raging
Railing against injustice.
It’s not fair for me
It’s not fair for you.
Join me in my struggle.
Unite in opposition.
Strengthen the struggle
(the cause devours its own baby)
United railing and rallying and raging
Against injustice.
Against –
Against –
Angst –
Angst ridden.
Suffering.
Suffering succotash, here again!
"In struggling against anguish one never produces serenity; the
struggle against anguish only produces new forms of anguish."
Simone Weil (1909-43), French philosopher, mystic. Draft of
letter to Andre Weil 1940 (published in Seventy Letters, pt. 2,
no. 39, 1965).
Sebastian Moore
The rejection of our common fate
Makes us strangers to each other,
The election of that fate,
In love, reveals us as one body.
PRESENT MOMENT
The Peace of Wild Things by Wendell Berry
When despair for the world grows in me
and I wake in the night at the least sound
in fear of what my life and my children's lives may be,
I go and lie down where the wood drake
rests in his beauty on the water, and the great heron feeds.
I come into the peace of wild things
who do not tax their lives with forethought
of grief. I come into the presence of still water.
And I feel above me the day-blind stars
waiting with their light. For a time
I rest in the grace of the world, and am free.
PRAYING by Mary Oliver
It doesn't have to be
the blue iris, it could be
weeds in a vacant lot, or a few
small stones; just
pay attention, then patch
a few words together and don't try
to make them elaborate, this isn't
a contest but the doorway
into thanks, and a silence in which
another voice may speak.
MINDFUL by Mary Oliver
Every day
I see or hear
something
that more or less
kills me
with delight,
that leaves me
like a needle
in the haystack
of light.
It was what I was born for -
to look, to listen,
to lose myself
inside this soft world -
to instruct myself
over and over
in joy,
and acclamation.
Nor am I talking
about the exceptional,
the fearful, the dreadful,
the very extravagant -
but of the ordinary,
the common, the very drab,
the daily presentations.
Oh, good scholar,
I say to myself,
how can you help
but grow wise
with such teachings
as these -
the untrimmable light
of the world,
the ocean's shine,
the prayers that are made
out of grass?
SELF AS CONTEXT
Eternity by William Blake
He who binds to himself a joy
Does the winged life destroy;
But he who kisses the joy as it flies
Lives in eternity’s sun rise.
On Wisdom and Perspective taking by Marcel Proust
We do not receive wisdom,
we must discover it for ourselves,
after a journey through the wilderness,
which no one else can make for us,
which no one can spare us,
for our wisdom is the point of view from which we come at last to regard the world.
WHERE WERE YOU LAST YEAR BY DAVID BRAZIER
Breath deep
Breath deep
The air fills my lungs and then?
My blood receives
This grace by which
I live a few moments more
My every cell replenished.
With every breath
A part of me departs
And something new
Is put in place.
The rice I ate yesterday,
Where is it now?
In my muscle, in my bone.
The juice we shared,
Where has it gone?
In our arms and legs and all.
Last month
The rice waved in the sunshine
In other lands:
In the low flood plains
Of the Mississippi
Or Irrawaddy;
And the fruit hung
On trees in Cyprus
Sicily or Spain.
And before that?
Before that their substance
Was in the soil,
Was in the air,
Was in the seas.
Was in the seas
Waiting to be gathered up
Waiting to soar up into the highest reaches of the sky,
Waiting to become rain.
You and I
Are mostly water.
Last year
Most of each of us
Was in the ocean.
We circulated together
In the Atlantic
Or Pacific perhaps,
For we are mostly water.
And that water was lifted
By sunshine heat
By the impact of photons
Cascading down
Beating upon the ocean’s face.
And every photon
Comes from the sun,
From the belly of the star;
You and I were stars last year.
We chased each other
In the turbulent heart of the sun.
So who was it that lived in your house last year?
And where will you be next week?
Who is your true friend and who your foe?
And who will you be next year?
Breath deep
Breath deep.
This air is me.
This air is you.
This air we share.
I give my substance to you and
You yours to me.
With each breath I am linked
In a single orbit
With the great forests.
My out breath is their food.
Their’s fills my lungs.
Last year
I was a tree
And the tree was me.
Each day
We gather up substance
And continue the task
Of endlessly
Remaking ourselves
From one another.
Each day
We discard a portion
And continue the cycle
Of endlessly
Returning ourselves
To others.
Day by day we change
And become one another,
The substance of the universe,
Stardust and all,
Passing through us each
And we through it.
Where were you last year?
Breath deep,
Breath deep.
KNOCK KNOCK by NeLi Martin
Tight, tight.
The mind wraps the idea.
Enfold
Enclose
Wrap
Rap, rap
Knock, knock.
Who’s there?
Enfolded
Enclosed
Wrapped tight?
(pause)
To listen
To open
To inquire
- who is in there?
……the armour of the mind pops
And crackles its release.
Opening out to the vista
Of silence.
KEEP ON KNOCKING - Rumi
Keep on knocking
'til the joy inside
opens a window
look to see who's there
WHOEVER FINDS LOVE - Rumi
Whoever finds love
beneath hurt and grief
disappears into emptiness
with a thousand new disguises
Call Me by My True Names - Thich Nhat Hanh
Do not say that I'll depart tomorrow
because even today I still arrive.
Look deeply: I arrive in every second
to be a bud on a spring branch,
to be a tiny bird, with wings still fragile,
learning to sing in my new nest,
to be a caterpillar in the heart of a flower,
to be a jewel hiding itself in a stone.
I still arrive, in order to laugh and to cry,
in order to fear and to hope.
The rhythm of my heart is the birth and
death of all that are alive.
I am the mayfly metamorphosing on the surface of the river,
and I am the bird which, when spring comes, arrives in time
to eat the mayfly.
I am the frog swimming happily in the clear pond,
and I am also the grass-snake who, approaching in silence,
feeds itself on the frog.
I am the child in Uganda, all skin and bones,
my legs as thin as bamboo sticks,
and I am the arms merchant, selling deadly weapons to
Uganda.
I am the twelve-year-old girl, refugee on a small boat,
who throws herself into the ocean after being raped by a sea
pirate,
and I am the pirate, my heart not yet capable of seeing and
loving.
I am a member of the politburo, with plenty of power in my
hands,
and I am the man who has to pay his "debt of blood" to, my
people,
dying slowly in a forced labor camp.
My joy is like spring, so warm it makes flowers bloom in all
walks of life.
My pain if like a river of tears, so full it fills the four oceans.
Please call me by my true names,
so I can hear all my cries and laughs at once,
so I can see that my joy and pain are one.
Please call me by my true names,
so I can wake up,
and so the door of my heart can be left open,
the door of compassion.
VALUES
Quote by Howard Thurman (American philosopher)
Don’t ask yourself what the world need; ask yourself what makes you come alive. And then go and do that. Because what the world need is more people who have come alive.
WILD GEESE by Mary Oliver
You do not have to be good.
You do not have to walk on your knees
For a hundred miles through the desert, repenting.
You only have to let the soft animal of your body
love what it loves.
Tell me about despair, yours, and I will tell you mine.
Meanwhile the world goes on.
Meanwhile the sun and the clear pebbles of the rain
are moving across the landscapes,
over the prairies and the deep trees,
the mountains and the rivers.
Meanwhile the wild geese, high in the clean blue air,
are heading home again.
Whoever you are, no matter how lonely,
the world offers itself to your imagination,
calls to you like the wild geese, harsh and exciting --
over and over announcing your place
in the family of things.
"All the True Vows" from The House of Belonging by David Whyte.
All the true vows
are secret vows
the ones we speak out loud
are the ones we break.
There is only one life
you can call your own
and a thousand others
you can call by any name you want.
Hold to the truth you make
every day with your own body,
don't turn your face away.
Hold to your own truth
at the center of the image
you were born with.
Those who do not understand
their destiny will never understand
the friends they have made
nor the work they have chosen
nor the one life that waits
beyond all the others.
By the lake in the wood
in the shadows
you can
whisper that truth
to the quiet reflection
you see in the water.
Whatever you hear from
the water, remember,
it wants you to carry
the sound of its truth on your lips.
Remember,
in this place
no one can hear you
and out of the silence
you can make a promise
it will kill you to break,
that way you'll find
what is real and what is not.
I know what I am saying.
Time almost forsook me
and I looked again.
Seeing my reflection
I broke a promise
and spoke
for the first time
after all these years
in my own voice,
before it was too late
to turn my face again.
Joanna Macy
As our awareness grows, so does that of the web,
for we are the universe becoming conscious of itself.
With sensibilities evolved through a millennia of interaction,
we can turn now and know that web as our home.
It both cradles us and calls us to weave it further.
COMMITTED ACTION
The Journey by Mary Oliver, from Dreamworld
One day you finally knew
what you had to do, and began,
though the voices around you
kept shouting
their bad advice –
though the whole house
began to tremble
and you felt the old tug
at your ankles.
“Mend my life!”
each voice cried.
But it didn’t stop.
You knew what you had to do,
though the wind pried
with it’s stiff fingers
at the very foundations,
though their melancholy
was terrible.
It was already late
enough, and a wild night,
and the road full of fallen branches and stones.
But little by little,
as you left their voices behind,
the stars began to burn
through the sheets of clouds,
and there was a new voice
which you slowly
recognised as your own,
that kept you company
as you strode deeper and deeper
into the world,
determined to do
the only thing you could do –
determined to save
the only life you could save.
Commitment - Aziza Sa'id
Commitment creates freedom.
When you commit to a movement,
you make it with your whole body.
When you commit to a feeling,
your passion will give power to your message.
When you commit to a dance,
your feeling reaches beyond your limitations.
When you commit to your path,
give yourself over to your way of growth, Magic happens...
obstacles get out of your way, mountains lay down before you,
the sky opens up above you,
and you will find yourself transformed.
Commitment - Goethe
"Until one is committed, there is hesitancy, the chance to draw back-- Concerning all acts of initiative (and creation), there is one elementary truth that ignorance of which kills countless ideas and splendid plans: that the moment one definitely commits oneself, then Providence moves too. All sorts of things occur to help one that would never otherwise have occurred. A whole stream of events issues from the decision, raising in one's favour all manner of unforeseen incidents and meetings and material assistance, which no man could have dreamed would have come his way. Whatever you can do, or dream you can do, begin it. Boldness has genius, power, and magic in it. Begin it now."
From “Little Gidding” – TS Eliot
We shall not cease from exploration
And the end of all our exploring
Will be to arrive where we started
And know the place for the first time.
...
A condition of complete simplicity
(Costing not less than everything)
And all shall be well and
All manner of thing shall be well
The Kookaburras - Mary Oliver (costs of not taking CA)
In every heart there is a coward and a procrastinator.
In every heart there is a god of flowers, just waiting
to stride out of a cloud and lift its wings.
The kookaburras, pressed against the edge of their cage,
asked me to open the door.
Years later I remember how I didn't do it,
how instead I walked away.
They had the brown eyes of soft-hearted dogs.
They didn't want to do anything so extraordinary, only to fly
home to their river.
By now I suppose the great darkness has covered them.
As for myself, I am not yet a god of even the palest flowers.
Nothing else has changed either.
Someone tosses their white bones to the dung-heap.
The sun shines on the latch of their cage.
I lie in the dark, my heart pounding.
COMMITMENT by NeLi Martin (costs of not taking CA)
Commitment tugs at my skirt edges,
Come on, you need me!
I gaze vacantly into the distance.
Make a joke.
Move on,
Pretending not to notice
The dragging at my hem line,
But all the while
feeling I’ve left something behind.
What We Knew - Carolyn Elkins from Daedalus Rising
At times we feel the need to go back
to plain things. To stones, earth,
grass, wind. To things we have known
a long time, to what we knew
when what filled the hours was dirt
and a few sticks, a pile of leaves
or some thin, white bones
from a long-dead bird.
The huge rock near the creek
was not too hard to lie on then
and the sun on bare skin felt warm.
We did not feel the press of time
as we do now. The world seemed firm
and real, and life was slow, and long, and good.
Michael Jordan
“I've missed more than 9000 shots in my career.
I've lost almost 300 games.
26 times I've been trusted to take the game winning shot ...
and missed.
I've failed over and over and over again in my life.
That is why I succeed.”
Lance Armstrong
The world is full of people who are trying to purchase self-confidence,
or manufacture it,
or who simply posture it.
But you can’t fake confidence,
you have to earn it.
If you ask me, the only way to do that is work.
You have to do the work.’
“Knowing trees, I understand the meaning of patience.
Knowing grass, I can appreciate persistence.” -
Hal Borland, journalist (1900-1978)
"And the day came when the risk to remain in a bud was greater
than the risk it took to blossom." Anais Nin
A Community of the Spirit - Rumi
There is a community of the spirit.
Join it, and feel the delight
of walking in the noisy street
and being the noise.
Drink all your passion,
and be a disgrace.
Close both eyes
to see with the other eye.
Open your hands,
if you want to be held.
Sit down in the circle.
Quit acting like a wolf, and feel
the shepherd's love filling you.
At night, your beloved wanders.
Don't accept consolations.
Close your mouth against food.
Taste the lover's mouth in yours.
You moan, "She left me." "He left me."
Twenty more will come.
Be empty of worrying.
Think of who created thought!
Why do you stay in prison
when the door is so wide open?
Move outside the tangle of fear-thinking.
Live in silence.
Flow down and down in always
widening rings of being.
I have Something to Say - NeLi Martin
I have SOMETHING to say.
Can you listen?
Will those fine bones
In your cochlear
Vibrate in a manner which will
Get your attention?
Will these vibrations
From my larynx
Fire your neurons
With a pattern of
Cognitive recognition?
Will you see you
In my words?
My neuron firing
Your neurons.
Can I make your acquaintance?
Arhh, a sea of expectant faces and this heart beats
Nervous to reveal…
And this heart rattles
At the cages of sinew and bone.
Can I get out of this skin?
To connect with you
Reach into your heart, feel
It beating
Like mine
Awaiting freedom from self consciousness
Waiting to connect
To everything. To be
Bound
To nothing,
And this heart beats
Nervous to reveal…..
And standing naked, this heart sees.
My friend, I see
I see your vulnerability
I see your vulnerability and my heart breaks
My heart breaks open
My heart breaks open and I walk
I walk on water
I drink the ocean
The ocean that is you and me
And everything we have ever been
And everything we have ever been is
Beautiful
Is love
Wendell Berry : "The Real Work" posted by Pete Bloom
It may be that when we no longer know what to do
we have come to our real work,
and that when we no longer know which way to go
we have come to our real journey.
The mind that is not baffled is not employed.
The impeded stream is the one that sings.
The Zebra Question, by Shel Silverstein
I asked the zebra,
Are you black with white stripes?
Or white with black stripes?
And the zebra asked me,
Are you good with bad habits?
Or are you bad with good habits?
Are you noisy with quiet times?
Or quiet with noisy times?
Are you happy with some sad days?
Or are you sad with some happy days?
Are you neat with some sloppy ways?
Or are you sloppy with some neat ways?
And on and on and on and on
And on and on he went.
I'll never ask a zebra
About stripes
Again.
Acceptance and Commitment Song
Acceptance and Commitment SongHello all!
This audio recording, available as either a link or download by ACBS members, is my attempt at capturing both the essence and spectrum of the psychological flexibility model in song-form. The recording is a bare bones acoustic/vocal version and the lyrics are below. Hope you enjoy! Lou Lasprugato
Acceptance and Commitment Song
There's suffering when you run away from pain
Expecting change but doing more of the same
And it's a long way down when your mind's pushing you around
Open up, open up
Step into this space
See what you need to face
To get through, to get through
What matters to you (2x)
It's hard when love's all but lost
And your best is not good enough
And you fill with fear when you're anywhere but here
As you move
As you sway
In the eye of the storm
In the depths of the pain
Will you take a stand?
Will you carry me?
Will you notice hurt?
Will you let it be?
Will you take a stand?
Will you carry me?
Will you notice love?
Will you let it be?
And breathe...
Fables for Parents
Fables for ParentsI've been inspired to write several 'fables' for parents - stories written to inspire vital living and loving, responsive parenting. Two of my fables in particular are grounded in Acceptance and Commitment Therapy and they are attached. All of my Fables for Parents can be freely distributed by any manner you like whatsoever. Just make sure that you say somewhere that I'm the author (Koa Whittingham) and give a link to my website www.koawhittingham.com.
Brianna's Life Mission illustrates experiential acceptance and committed action in the context of parenting
Ashley's True Self explores self-as-context in a manner relvant to parents
If you'd like to read more Fables for Parents then check out my website: http://www.koawhittingham.com/fables-for-parents/
Quotes with an ACT Theme
Quotes with an ACT ThemeThese quotes, most of which are good to share with clients, come from numerous resources, including the introductory quotes to chapters of ACT books.
If you have more to add, add a comment or child page and they'll be added.

We cannot change anything until we accept it. Condemnation does not liberate, it oppresses. — Carl Jung
The mystery of life is not a problem to be solved, but a reality to be experienced. — Zen Saying
If you don't know where you are going, you might not get there. — Yogi Berra
Life is what happens to you while you're busy making other plans. — John Lennon
Right now a moment of time is passing by!... We must become that moment. — Paul Cezanne
Although the world is full of suffering, it is full also of the overcoming of it. — Helen Keller
The significant problems we face cannot be solved at the same level of thinking we were at when we created them. — Albert Einstein
The only way out is through. — Robert Frost
If we all worked on the assumption that what is accepted as true is really true, there would be little hope of advance. — Orville Wright
It takes courage to grow up and turn out to be who you really are. — e. e. cummings
Live as if you were to die tomorrow. Learn as if you were to live forever. — Gandhi
Our greatest glory is not in never failing, but in rising every time we fall. — Confucius
Pay no attention to the man behind the curtain. — The Wizard of Oz
When suffering knocks at your door and you say there is no seat for him, he tells you not to worry because he has brought his own stool. — Chinua Achebe
I used to think that the brain was the most wonderful organ in my body. Then I realized who was telling me this. — Emo Phillips
Our one true home is in the present moment. — Thich Nhat Hanh
You can observe a lot just by watching. — Yogi Berra
When I dare to be powerful, to use my strength in the service of my vision, then it becomes less important whether I am afraid. — Audre Lorde
It takes a deep commitment to change and an even deeper commitment to grow. — Ralph Ellison
When you begin to touch your heart or let your heart be touched, you begin to discover that it's bottomless, that it doesn’t have any resolution, that this heart is huge, vast and limitless. You begin to discover how much warmth and gentleness is there, as well as how much space. — Pema Chodron
When you change the way you look at things, the things you look at change. — Wayne Dyer
It's like you're surfing… The same wave that can be a source of pain can be a beautiful flowing grace and source of power. It's all a matter of how you respond to it. — Trey Anastasio
It is only by practicing through a continual succession of agreeable and disagreeable situations that we acquire true strengths. To accept that pain is inherent and to live our lives from this understanding is to create the causes and conditions for happiness. — Suzuki Roshi
Seventy percent of success in life is showing up. — Woody Allen
In the end it's not the years in your life that count. It's the life in your years. — Abraham Lincoln
He is no fool who gives what he cannot keep to gain what he cannot lose. — Jim Elliot
Any emotion, if it is sincere, is involuntary. — Mark Twain
Life moves pretty fast. If you don't stop and look around once in a while, you could miss it. — Ferris Bueller
Be the change you wish to see in the world. — Gandhi
All life is an experiment. The more experiments you make the better. — Ralph Waldo Emerson
Experience is the teacher of all things. — Julius Caesar
In order for the light to shine so brightly, the darkness must be present. — Sir Francis Bacon
If we have no peace, it is because we have forgotten that we belong to each other. — Mother Teresa
If there is no struggle, there is no progress. — Frederick Douglass
Humor is mankind's greatest blessing. — Mark Twain
Make each day your masterpiece. — John Wooden
Never despair; but if you do, work on in despair. — Edmund Burke
When you come to a fork in the road, take it. — Yogi Berra
You can hold yourself back from the sufferings of the world, this is something you are free to do and is in accordance with your nature, but perhaps precisely this holding back is the only suffering that you might be able to avoid. — Franz Kafka
Uncertainty is not a pleasant condition; but certainty is absurd. — Voltaire
Fear doesn't go away but you walk toward fear naked and the gate opens. — Starhawk
When a great ship is in harbor and moored, it is safe, there can be no doubt. But that is not what great ships are built for. — Clarissa Pinkola Estes
You can't stop the waves, but you can learn to surf. — Joseph Goldstein
Do not look back in anger, or forward in fear, but around in awareness. — James Thurber
Now and then it's good to pause in our pursuit of happiness and just be happy. — Guillaume Apollinaire
The truth that many people never understand, until it is too late, is that the more you try to avoid suffering the more you suffer because smaller and more insignificant things begin to torture you in proportion to your fear of being hurt. — Thomas Merton
The civilized man has built a coach, but has lost the use of his feet. — Ralph Waldo Emerson
It is impossible to live without failing at something, unless you live so cautiously that you might as well not have lived at all - in which case, you fail by default. — J.K. Rowling
You can close your eyes to the things you don't want to see, but you can't close your heart to the things you don't want to feel. — Unknown
It's not the load that breaks you down, it's the way you carry it. — Lena Horne
Blessed are the flexible, for they shall not be bent out of shape. — Anonymous
Do or do not. There is no try. — Yoda (Star Wars)
I've been absolutely terrified every moment of my life - and I've never let it keep me from doing a single thing I wanted to do. — Georgia O'Keeffe
Life is not tried, it is merely survived if you're standing outside the fire. — Garth Brooks
The dogmas of the quiet past are inadequate to the stormy present. — Abraham Lincoln
Do one thing every day that scares you. — Eleanor Roosevelt
In the beginning the universe was created. This has made a lot of people very angry and been widely regarded as a bad move. — Douglas Adams
Humans think they are smarter than dolphins because we build cars and buildings and start wars etc… and all that dolphins do is swim in the water, eat fish and play around. Dolphins believe that they are smarter for exactly the same reasons. — Douglas Adams
Wisdom and compassion flow from simplicity and clarity; from having nothing to prove and nothing to defend. — Barry Magid
Rumi Quotes
Rumi Quotes
“Be empty of worrying.
Think of who created thought!
Why do you stay in prison
When the door is so wide open?"
“These pains you feel are messengers. Listen to them.”
“Brother, stand the pain.
Escape the poison of your judges.
The sky will bow to your beauty, if you do.
Learn to light the candle. Rise with the sun.
Turn away from the cave of your sleeping.
That way a thorn expands to a rose."
“Are you jealous of the ocean’s generosity?
Why would you refuse to give this joy to anyone? Fish don’t hold the sacred liquid in cups! They swim the huge fluid freedom.”
"Come, come, come whatever you are..
Good or bad,
It doesn't matter.
Ours is not a caravan of despair.
Come, even if you have broken your vow a thousand times
Come, yet again, come, come."
"Submit to love without thinking"
"Close your eyes, fall in Love, stay there."
"When love itself comes to kiss you, don’t hold back!"
"Speak with the language of love."
"If the house of the world is dark, Love will find a way to create windows."
"Love is a silent language."
"Love will find its way through all languages on its own."
"As you live deeper in the heart, the mirror gets clearer and cleaner."
"Now’ is where love breathes."
"No words can explain how inspired words spring out of silence."
"Free yourself from your own thoughts."
"Enough of words. Come to me without a sound."
"Sit, be still, and listen."
"Hear the passage into silence and be that."
"You are the seeker, the goal, and seeking itself. Not only a part of them"
"Don’t sit and wait. Get out there, feel life. Touch the sun, and immerse in the sea."
"Give yourself a kiss. If you want to hold the beautiful one, hold yourself to yourself."
"You are not a drop in the ocean. You are the entire ocean in a drop."
"We often need to be refreshed."
"The moment you accept what troubles you’ve been given, the door will open."
"Respond to every call that excites your spirit."
"Everything about yesterday has gone with yesterday. Today, it is needed to say new things."
"If you are irritated by every rub, how will you be polished?."
"Don’t grieve, anything you lose comes round in another form."
"Smiles come best from those who weep."
"Do not be satisfied with the stories that come before you. Unfold your own myth."
"Stay in the spiritual fire. Let it cook you."
Customizable ACT Toolkit
Customizable ACT ToolkitJust wanted to share a free customizable toolkit I created! It keeps all my favorite interventions, resources, and tools handy:
✨ Simplifies session planning
✨ Streamlines recommending curated resources to clients
✨ Helps you pick the perfect ACT intervention or metaphor instantly
→ Check it out and make it your own!
How to Simply Explain Out of Network Benefits to Clients
How to Simply Explain Out of Network Benefits to ClientsWorried folks might click away when they see you're out-of-network?
I got your back- a clear, friendly breakdown of OON benefits can keep them sticking around to see why you’re worth it and ease worries about the whole OON process.
Not sure how to explain those benefits without drowning in jargon that even confuses you sometimes?
Grab Your Free Copy of: Explaining OON Benefits: Essential swipe Copy
✨ Ready-to-Use Explanations
✨Process Breakdown
✨Reassurance Tips
✨Helpful Tools
Marketing Materials
Marketing MaterialsThis section is for sharing materials used to market ACT services, ideas, trainings, etc.
An example brochure on an ACT-focused treatment program
An example brochure on an ACT-focused treatment programBuild Connections & Boost Referrals: Networking Spreadsheet
Build Connections & Boost Referrals: Networking Spreadsheet- Keep Track of Your Go-Tos
- From your work bestie to your “I wish they were my mentor,” keep all your faves in one spot.
- Collab Dreams
- Spot chances to collaborate on stuff that’s close to your heart and practice.
- Share the Wisdom
- Swap tools, tips, and “aha” moments that can make everyone’s practice shine.
- Boost Your Referrals
- Make giving and getting referrals a breeze, expanding your network and client base with the right connections.
✨ Check it out here ✨
Example brochure for ACT in collaboration with primary care physicians
Example brochure for ACT in collaboration with primary care physiciansRobert Purssey donated the sample flyer below that he has used in his practice and says that people are free to borrow it and modify it for their own use.
How to Write Your About Page (free workbook)
How to Write Your About Page (free workbook)Here’s what you’ll get-
→ 50+ Curated Questions: Dive into an expansive selection of over 50 questions designed to ease the process of crafting your about page.
→ Writing Tips and Advice: This guidance is aimed at forging a genuine connection with your ideal clients, ensuring that your narrative resonates with those who would be the best fit for you.
→ 12 Key About Page Elements: Uncover the 12 critical components that every compelling about page should include.
✨Check it out here✨
Using the Hexaflex in publications - Copyright
Using the Hexaflex in publications - CopyrightFrom Steve Hayes 24 October, 2017:
When people ask I say it [the hexaflex] can be used at no cost or restrictions but it should be done with the attribution "Copyright Steven C. Hayes. Used by permission."
I list it that way myself, when I use it.
Steven C. Hayes
☺️ Free ACT Website Copy
☺️ Free ACT Website Copy
✨FAQ section
✨"My Approach" section and
✨ ACT headlines to sprinkle throughout your site
→ Get the free ACT Website Copy here

Smartphone Apps
Smartphone Apps
The ACTing with Technology SIG resources webpage has a list of smartphone apps. ACBS members can access the webpage here
The ACTing with Technology SIG has a website, which includes a section about Apps and Websites.
ACT for Special Populations
ACT for Special Populations- ACT for Law Enforcement
- ACT for Sport
- Acceptance and Commitment Therapy for Insomnia (ACT-I) by Dr Guy Meadows
- Bible resources for Christian clients
- Research on ACT and Islam
- ACT with Children, Adolescents, Parents, Teachers, Etc.
- ACT in the US Department of Veterans Affairs
- ACT in Private Practice
Other Resources on the ACBS website
There are several Special Interest Groups (SIGs) focused on specific populations and settings. This is a partial list of SIGs. To see the full list of SIGs, click here.
- ACT and Autism SIG
- ACT for Military SIG
- ACT in Education
- ACT in Perinatal
- ACT in Primary Care SIG
- Aging in Context SIG
- Applying ACT to Addictions SIG
- CBS and Cancer SIG
- Children, Adolescents & Families SIG
- College/University Student Mental Health SIG
- Coaching SIG
- Contextual Medicine SIG
- Forensic and Corrections SIG
- Gender and Sexual Diversity SIG
- Occupational Therapy & ACT SIG
- OCD and Related Disorders SIG
- Pain SIG
- Physiotherapy SIG
- Psychosis SIG
- Sport, Health, and Human Performance SIG
- Veterans Affairs (VA) ACT SIG
ACT with Children, Adolescents, Parents, Teachers, Etc.
ACT with Children, Adolescents, Parents, Teachers, Etc.Resources on the ACBS Website
- ACT-Related Measures (Child and Adolescent Specific)
- Treatment Protocols and Manuals for Children, Adolescents, and Parents
- ACT in Schools
- ACT in Context Podcast Episode 11: ACT with Adolescents with Dr. Louise Hayes
- Miscellaneous Resources
- Children, Adolescents, and Families SIG Resource Toolbox (Available to ACBS members only)
There are Special Interest Groups (SIGs) that ACBS members can join:
- Children, Adolescents and Families SIG
- ACT and Autism SIG
- College/University Student Mental Health SIG
- ACT in Education SIG
- ACT in Perinatal SIG
Therapist guides
- Challenging Perfectionism: An Integrative Approach for Supporting Young People Using ACT, CBT and DBT (2020) by Dawn Starley
- Acceptance and Commitment Therapy: The Clinician's Guide for Supporting Parents (2019) by Koa Whittingham and Lisa Coyne
- Parenting a Troubled Teen: Manage Conflict and Deal with Intense Emotions Using Acceptance and Commitment Therapy (2017) by Patricia E. Zurita Ona PsyD
- EMPOWER Your Students: Tools to Inspire a Meaningful School Experience (2017) book by Lauren Porosoff and Jonathan Weinstein
- Acceptance & Mindfulness Treatments for Children & Adolescents: A Practitioner’s Guide
- ACT for Adolescents: Treating Teens and Adolescents in Individual and Group Therapy
- Mindfulness and Acceptance for Counseling College Students: Theory and Practical Applications for Intervention, Prevention, and Outreach (The Context Press Mindfulness and Acceptance Practical Series)
- Teen Anxiety: A CBT and ACT Activity Resource Book for Helping Anxious Adolescents
- The Thriving Adolescent: Using Acceptance and Commitment Therapy and Positive Psychology to Help Teens Manage Emotions, Achieve Goals, and Build Connection
Client books
- Acceptance and Mindfulness Toolbox for Children and Adolescents: 75+ Worksheets & Activities for Trauma, Anxiety, Depression, Anger & More
- The ACT Workbook for Teens with OCD
- Becoming Mum
- Dark Agents, Book One: Violet and the Trial of Trauma
- EMPOWER Your Students: Tools to Inspire a Meaningful School Experience, Grades 6-12
- Get Out of Your Mind and Into Your Life for Teens: A Guide to Living an Extraordinary Life
- The Gifted Kids Workbook: Mindfulness Skills to Help Children Reduce Stress, Balance Emotions, and Build Confidence
- The Joy of Parenting: An Acceptance and Commitment Therapy Guide to Effective Parenting in the Early Years
- The Mental Health and Wellbeing Workout for Teens: Skills and Exercises from ACT and CBT for Healthy Thinking
- The Mindfulness and Acceptance Workbook for Teen Anxiety: Activities to Help You Overcome Fears and Worries Using
- Acceptance and Commitment Therapy (Instant Help Book for Teens)
- Nuna and the Fog
- Parenting a Troubled Teen: Manage Conflict and Deal with Intense Emotions Using Acceptance and Commitment Therapy
- Parenting Your Anxious Child with Mindfulness and Acceptance: A Powerful New Approach to Overcoming Fear, Panic, and Worry Using Acceptance and Commitment Therapy
- Stuff That Sucks: Accepting What You Can’t Change and Committing to What You Can
Miscellaneous Resources
Miscellaneous ResourcesACT For Kids: Living a Valued Life
ACT For Kids: Living a Valued LifeThis ACT for Kids manual was developed by Steven Gordon, Michael Asher, and Michael Selbst
Please note: due to copyright laws, ACBS removed images from the document. Therefore, some of the formatting might be slightly off.
ACT in College Counseling -- Book Interview
ACT in College Counseling -- Book InterviewIn this interview (2013), psychologist Dr. Jacqueline Pistorello discusses the latest research on challenges faced by college students, as well as new attempts at supporting them with mindfulness and acceptance interventions. In her recently editted book, Mindfulness and Acceptance for Counseling College Students, Pistorello and others explore how mindfulness and acceptance-based approaches such as acceptance and commitment therapy (ACT), dialectical behavioral therapy (DBT), mindfulness-based cognitive therapy (MBCT), and mindfulness-based stress reduction (MBSR) are being utilized in higher education settings around the world to treat student mental health problems like severe depression, substance abuse, and eating disorders, and/or to help students thrive--both in and out of the classroom.
Q: Are college students more distressed these days?
For adults whose idea of college is this carefree time full of fun and little adult pressures, the current statistics on college mental health may be startling. Suicide is one of the leading causes of death among college students (Suicide Prevention Resource Center, 2004). Over 20% of college students have seriously considered suicide and 8% have attempted it in their lifetime (American College Health Association (ACHA), 2012). Non-suicidal self-injury (NSSI) is also prevalent: 15.3% have engaged in it in their lifetime and 6.8% in the past year (Whitlock et al., 2011). Nearly 50% of college students have a diagnosable psychiatric disorder (Blanco et al., 2008); one in five has suffered from depression and two out of three have experienced overwhelming anxiety in their lifetime (ACHA, 2012). Severe drinking problems are common, with one third engaging in binge drinking (Wechsler & Kowalik, 2005) and 20% experiencing an alcohol use disorder (Blanco et al., 2008); college students are more likely to drink and drive, to engage in binge drinking, and less likely to seek treatment for substance abuse, than their college-aged counterparts in the community.
The question of whether this is an actual increase in pathology is being debated, but the data are compelling. One study examined birth cohort increases in psychopathology among young Americans and demonstrated that American high school and college students reported a gradual increase of symptoms of psychopathology relative to previous generations over the last 70 years, with the current generation of young adults scoring about a standard deviation higher on clinical scales. University counseling center directors overwhelmingly state that the number of college students seeking mental health treatment for serious concerns at counseling centers is increasing. One study showed that the percentage of students presenting with depression, suicidality, and personality disorders doubled within a decade (Benton, Robertson, Tseng, Newton, & Benton, 2003).
Q: Do we need to think differently when treating college students specifically? Aren't college students the same as adolescents or adults, depending on their age?
Traditional college students fall into a special category developmentally. The period between the ages of 18-26 has recently been coined as “emerging adulthood” (Arnett, 2000). This age bracket encompasses the majority of undergraduate students in Universities in the US and even abroad. Researchers have shown that this stage of development is different from adolescence, in that it is characterized by fast transitions into novel and varied social contexts bringing greater freedom and less social control than experienced during adolescence. College students face special pressures as well: a greater proportion live away from home and they are pressed to do well academically; to live up to parents’ expectations; to co-exist with other students, sometimes in very closed quarters; to become more comfortable with those who hail from different socio-cultural-economic backgrounds; to figure out where one stands in terms of sexual orientation, religion, politics, and so on. Thus, what may work with adolescents may not work with this population. Some studies have found, for example, that factors affecting the trajectory of substance abuse among adolescents differ for those in emerging adulthood.
In addition to developmental issues affecting traditionally aged college students, the treatment of students, traditional and non-traditional (students who return to college at an older age), within the context of a campus pose unique challenges. The “therapist” working at a College Counseling Center has a broader role than might typically be expected, balancing mental health and educational issues, balancing the student’s individual needs with campus safety, having to manage confidentiality in the context of parent phone calls, dealing with administrators’ inquiries, and so on.
Understanding how different approaches can be implemented with emerging adults and within a college context, can be very useful to clinicians and researchers alike.
Q: We understand that you have an edited book coming out on mindfulness and acceptance in counseling college students, by New Harbinger. Why are mindfulness and acceptance important for college students?
That’s a great question. It used to be the case that people could limit their exposure to the amount and kind of information. These days, particularly because of technology, the world moves very fast (e.g., constant texting, Tweeting, rapid video games, multi-tasking) and we are bombarded with a steady stream of information, sometimes gruesome pictures that stay in our minds. We can probably all still picture the planes going into the Twin Towers or more recently, the two blasts during the Boston Marathon bombings. Social networks like Facebook also promote constant comparisons among young adults, and some of their most private matters, sometimes in the context of cyber bullying, may be revealed en masse in ways that cannot be taken back. Unlike those of us who are middle aged now, typical college kids are growing up this way, and we don’t know what effect this will have on their mental health. The research on experiential avoidance is virtually undisputed, suggesting that unless emergent adults learn ways to bring their attention back to this present moment and be able to “carry” difficult emotions, memories, urges, and thoughts, including perhaps constant self-judgments, the repercussions are likely to be dire.
Mindfulness and acceptance-based approaches have something to offer emerging adults that might very well not only be unique but utterly necessary given the current socio-cultural context.
Q: So, tell us a little about your book. What is it? What mindfulness approaches are discussed in it?
This is an edited “how to” book. It provides illustration of how different mindfulness and acceptance-based approaches are being utilized with college students. A thorough review of specific mindfulness based approaches with college students at this point would be premature. Although this is a burgeoning field, and more and more studies are being conducted every month, the empirical evidence specifically with college students is building. The book emphasizes ACT, it also provides exposure to how DBT, MBSR, MBCT, and Ellen Langer’s mindful learning can be applied with college students and/or campus settings. This book is primarily geared towards practitioners or researchers working with college students or young adults. However, the book may be useful for anyone trying to implement ACT or other mindfulness based approaches outside the more typical therapy setting. The chapters are diverse and some of the initiatives go outside the box and may be helpful to individuals who are entertaining applying ACT or mindfulness based approaches in different settings.
This is a practical guide. The chapters are written by extremely knowledgeable authors who are not just theoreticians but are "in the trenches" and know how to explain what works best in a very practical, step-by-step way. The book also includes an extensive online Appendix where protocols, Power Point presentations, and modifiable Word documents (e.g., group flyers) developed by chapter authors can be accessed; this can be a huge time saver.
Q: What new research is included that will be of interest to the ACT community?
We do have some hot off the press research findings mentioned in this book, hailing from across the globe (Australia, Italy, England, and the United States), that will be of interest to the ACT community in general. For example, one of the chapters summarizes findings from a study comparing ACT and MBCT. Although there were almost no differences in outcome, the authors discuss which individuals may benefit more from each approach. Another chapter described ACT podcasts that were created for college students, and summarizes findings regarding the utility of ACT podcasts, relative to CBT podcasts; this study found that students listening to the ACT podcasts reported greater academic engagement (e.g., less reading/texting during classes). Another chapter described a transdiagnostic ACT group showing promising findings; although we often laud ACT for being a transdiagnostic approach, most published ACT research so far has focused on one specific diagnostic categories (e.g., depression, psychosis), whereas this open trial study included a range of anxiety and mood problems. Other chapters describing ACT have gone beyond the therapy room, such as applying ACT in various classroom settings (including infusing ACT into an Abnormal Psychology class or creating ACT seminars), towards the training of college student peer mentors, and via an online values intervention. The latter study showed that adding values training to an online goal-setting procedure led to statistically significant improvements in grades. The range of new approaches and methods is impressive and readers will have a lot of new ideas about how to best serve college students.
ACT in Schools
ACT in SchoolsACBS has an ACT in Education Special Interest Group (SIG) that members can join. Read more about the ACT in Education SIG and its mission here. The ACT in Education SIG has a SIG resources webpage available to ACBS members.
Below are members' discussions of ACT applications in specific settings and populations.
- Connect - Wellbeing from the Word Go (for Elementary/Primary School)
- Blind Spots: Why Students Fail and the Science That Can Save Them (2020) book by Kimberly Nix Berens
- Two-for-one Teaching: Connecting Instruction to Student Values; Integrate Social-emotional Learning into Academic Instruction (2019) book by Lauren Porosoff and Jonathan Weinstein
- Using ACT and RFT in the Classroom
- Finding the Door to the CBS House: How a Teacher Discovered ACT and Now Uses CBS in Her Classroom (ACBS Newsletter, October 2017)
- EMPOWER Your Students: Tools to Inspire a Meaningful School Experience, Grades 6-12 (Increase Motivation and Engagement in the Classroom) (2017) by Lauren Porosoff and Jonathan Weinstein
- Seven Session Protocol for Anti-bullying in Schools
- The Story of Little Sapling. by Dennis Embry and Leslie Rogers. This story is for children over age 6.
- Blog Post about ACT in Schools Research (2016)
- Blog Post about First Spanish Book on ACT Applied to Education (2014)
Connect - Wellbeing from the Word Go (Elementary/Primary School)
Connect - Wellbeing from the Word Go (Elementary/Primary School)April 2020
Over the past 2-3 years, a small group of colleagues and I have been developing a children’s psychological flexibility/wellbeing curriculum for the primary phase of education (4-11 years). The curriculum structure is such that:
* Each one of the six terms in a school year has a theme that is aligned with one or other of the New Economics Foundation’s (NEF’s Five Ways to Wellbeing: Exercise; Give to Others, Connect with Others; Challenge Yourself; and Embrace the Moment. One further theme has been added to make up the sixth term for the year. This theme is around Self-Care, which also featured strongly in the NEF’s (2008) analysis.
* Each lesson, within any given term, focuses on developing one or other of the six core wellbeing skills outlined in Louise Hayes and Joseph Ciarrochi's DNA-V model (2015)
For anyone interested, you can sign up to access a free trial here: https://www.connect-pshe.org/sign-up. This is immediately accessible as soon as you sign up for the free trial, which also includes a sample of lesson plans and associated ppt slides, handouts and other relevant resources. Please do feel free to pass on to any teachers, schools or other interested parties you think might be interested.
Overall, the curriculum consists of around 250 Connect-branded lesson plans, each with ppt sides, handouts and resources. The whole product is housed online, to reduce the use of paper, and therefore reduce Connect’s carbon footprint. Lesson plans follow the same basic structure, so teachers can quickly become familiar with how lessons are run. They are generally between 1000 and 1500 words, so plenty of detailed explanations built in.
For UK based recipients of this email, it’s also probably worth mentioning that the Connect PSHE wellbeing curriculum addresses all of the new DfE statutory requirements for PSHE Curriculums at the primary phase. We’ve designed the curriculum in this way in order to address two very closely related, important and relatively recent developments in government guidance for schools:
1. The new statutory requirements to deliver PSHE curriculums (2019): Relationship Education, Relationship and Sex Education and Health Education.
2. The expectation that schools will be front and centre of a national effort to improve children’s wellbeing, in line with the children’s mental health green paper (Dec 2017): Transforming Children and Young People’s Mental Health Provision.
The dream for this curriculum is that all children will have the opportunity to learn key wellbeing skills, proactively and preventatively, based on the best possible developmentally sensitive understanding the science of human wellbeing.
We really hope that schools, children, families and colleagues within our ACBS community will find the Connect wellbeing curriculum a useful resource for developing psychological flexibility skills with children.
I also just want to recognise the incredible help and support - in so many forms - during the development of this curriculum from Louise Hayes and Joseph Ciarrochi and so many other wonderful members of the ACBS community. It is a wonderful privilege to be part of such a kind, supportive, collaborative community.
Here's a link to the home page: www.connect-pshe.org
Best wishes,
Duncan and the rest of the Connect Team (Nic Hooper, Freddy Jackson-Brown, Corinna Grindle, Katie Parker & Emily Goyen)
Teacher's Guide to Evolution, Behavior, and Sustainability Science
Teacher's Guide to Evolution, Behavior, and Sustainability ScienceHumans are a highly cooperative species - cooperation is what brought us to the global society that we are today. And yet, the biggest problems facing the well-being of individuals, our species, and our planet seem to be the result of our inability to work together.
Humans are a highly flexible species - we inhabit almost all the ecosystems of the world. And yet, the biggest problems facing the well-being of individuals, our species, and our planet, seem to be the result of our inability for flexible behavior change.
How can teachers engage students in these apparent paradoxes?
The second edition of the Global ESD creative commons publication, A Teacher's Guide to Evolution, Behavior, and Sustainability Science, provides educators with an interdisciplinary road map to understanding the origins, development, and flexibility of our uniquely elaborated human capacities to cooperate around things that matter, and provides tools and approaches for teaching about these concepts in their classrooms.
Download the teacher guide here: http://guide.openevo.net
- Contributed by ACBS Member, Dr. Susan Hanisch (October 2020)

ACT with Children &/or Parents: State of the Research Address - ACBS World Conference II (2006)
ACT with Children &/or Parents: State of the Research Address - ACBS World Conference II (2006)Hi all.
I am attaching a Word file that provides information about ACT and/or ACT-related work with youth. There are some quick to review charts and lists, manuscript summaries, and references, as well as contact information for individuals working with "kiddos" or parents, teachers, etc. There is some admitted overlap and also some non-repetition between those things - so, for example, some (but not all) of the stuff listed in charts is listed in summaries and some citations are in summaries but not the reference list, etc. I ask that you just read it all carefully and overlook the imperfections. One of my students (Andrew Scherbarth) and I spent a good deal of time and have worked quite hard to get it looking as good as is does. A lot of information is there. We have excluded work that is only basic in nature. Therefore, it does not address RFT, stimulus equivalence studies, or the like UNLESS there was a clear clinical application in the title or abstract of the article, chapter, etc. I think that would be a great addition to the RFT section of this website (hint, hint). We are doing some of that in my lab now and may get around to posting it later, but if someone else could do it sooner... We did include in-press, in-review, in-preparation, ongoing, and even upcoming studies that I know of in addition to the published stuff. We included people doing clinical work without research components, but not in much detail. I did my best to include everything and mention everybody that I know has done or is doing this work. Please, please, forgive me if I forgot anything/anyone. If I wrongly included you, or you don't want to be included, I apologize. Please, let us all know. Also, if I did not know about you/your work and it should be included, please, take an active role in speaking and stepping up. We need more ACT stuff with these groups! What I hope is that people interested in clinical or research work with youth and related populations will "make themselves known" by adding their contact information and interests to this list. Ideally, new communication will be fostered and known contacts will be stregthened in efforts to advance this work. I provided some suggestions at WorldCon2 about where I think we need to go. If you take up those topics or others with youth, please let us all know!
Thanks and take care,
Amy Murrell (2006)
Full list of books for Children, Adolescents, and Parenting
Full list of books for Children, Adolescents, and ParentingTherapist guides
- Challenging Perfectionism: An Integrative Approach for Supporting Young People Using ACT, CBT and DBT (2020) by Dawn Starley
- Acceptance and Commitment Therapy: The Clinician's Guide for Supporting Parents (2019) by
- Acceptance & Mindfulness Treatments for Children & Adolescents: A Practitioner’s Guide
- ACT for Adolescents: Treating Teens and Adolescents in Individual and Group Therapy
- Mindfulness and Acceptance for Counseling College Students: Theory and Practical Applications for Intervention, Prevention, and Outreach (The Context Press Mindfulness and Acceptance Practical Series)
- Teen Anxiety: A CBT and ACT Activity Resource Book for Helping Anxious Adolescents
- The Thriving Adolescent: Using Acceptance and Commitment Therapy and Positive Psychology to Help Teens Manage Emotions, Achieve Goals, and Build Connection
Client books
- Acceptance and Mindfulness Toolbox for Children and Adolescents: 75+ Worksheets & Activities for Trauma, Anxiety, Depression, Anger & More
- The ACT Workbook for Teens with OCD
- Becoming Mum
- Dark Agents, Book One: Violet and the Trial of Trauma
- EMPOWER Your Students: Tools to Inspire a Meaningful School Experience, Grades 6-12
- Get Out of Your Mind and Into Your Life for Teens: A Guide to Living an Extraordinary Life
- The Gifted Kids Workbook: Mindfulness Skills to Help Children Reduce Stress, Balance Emotions, and Build Confidence
- The Joy of Parenting: An Acceptance and Commitment Therapy Guide to Effective Parenting in the Early Years
- The Mental Health and Wellbeing Workout for Teens: Skills and Exercises from ACT and CBT for Healthy Thinking
- The Mindfulness and Acceptance Workbook for Teen Anxiety: Activities to Help You Overcome Fears and Worries Using
- Acceptance and Commitment Therapy (Instant Help Book for Teens)
- Nuna and the Fog
- Parenting a Troubled Teen: Manage Conflict and Deal with Intense Emotions Using Acceptance and Commitment Therapy
- Parenting Your Anxious Child with Mindfulness and Acceptance: A Powerful New Approach to Overcoming Fear, Panic, and Worry Using Acceptance and Commitment Therapy
- Stuff That Sucks: Accepting What You Can’t Change and Committing to What You Can
(This webpage was updated on August 16, 2020)
Quick Tips for Parents
Quick Tips for ParentsThe following ACT consistent parenting tips are from Louise Shepherd and written with the general public in mind. Please feel free to share this with clients or friends, family etc.
Treatment Protocols and Manuals for Children, Adolescents, and Parents
Treatment Protocols and Manuals for Children, Adolescents, and ParentsTreatment Protocol and Manuals
- At-Risk Adolescents
- ACT for outpatient adolescent substance treatment
- ACT For Kids: Living a Valued Life
- ACT for Parents of Developmentally Disabled Children Manual
- Experiential Adolescent Group Program
- Mindtrain- ACT treatment manual for therapists working with anxious children
- Young Children
ACT in the US Department of Veterans Affairs
ACT in the US Department of Veterans AffairsThere are Special Interest Groups (SIGs) that ACBS members can join:
The April 2016 VA/DoD Clinical Practice Guideline for the Management of Major Depressive Disorder recommends ACT as a "first-line treatment for uncomplicated mild to moderate MDD", citing the research evidence for this recommendation as "strong"
http://www.healthquality.va.gov/guidelines/MH/mdd/MDDCPGClinicianSummaryFINAL5192016.pdf
Articles from Journal of Contextual Behavioral Science (JCBS) pertinent to ACT in the VA:
- O'Brien, K., Dozier, M., Lopez, J., & Ruha, A. (2021) A new treatment model for veterans?: Results from a program evaluation of a recovery-oriented intensive outpatient program for veterans with heterogeneous diagnostic presentations. JCBS, Vol. 19, Pages 57-63. https://doi.org/10.1016/j.jcbs.2020.12.001
- Wharton, E., Sears Edwards K., Juhasz, M., and Walser, R. (2019). Acceptance-based interventions in the treatment of PTSD: Group and individual pilot data using Acceptance and Commitment Therapy. JCBS, Vol. 14, 55-64.
- Cox, D. W., Motl, T. C., Bakker, A. M., & Lunt, R. A. (2018). Cognitive fusion and post-trauma functioning in veterans: Examining the mediating roles of emotion dysregulation. JCBS, Vol. 8, 1-7.
- Farnsworth, J. K., Drescher, K. D., Evans, W., Walser, R. D. (2017). A functional approach to understanding and treating military-related moral injury. JCBS, Vol. 6, Issue 4, 391-397.
- Cobb, A. R., Lancaster, C. L., Meyer, E. C., Lee, H., & Telch, M. J. (2017). Pre-deployment trait anxiety, anxiety sensitivity and experiential avoidance predict war-zone stress-evoked psychopathology. JCBS, Vol. 6, Issue 3, 276-287. doi:10.1016/j.jcbs.2017.05.002
- Hermann, B. A., Meyer, E. C., Schnurr, P. P., Batten, S. V., & Walser, R. D. (2016). Acceptance and commitment therapy for co-occurring PTSD and substance use: A manual development study. JCBS, Vol. 5, Issue 4, 225-234.
- Bryan, C. J., Ray-Sannerud, B., Heron, E. A. (2015). Psychological flexibility as a dimension of resilience for posttraumatic stress, depression, and risk for suicidal ideation among airforce personnel. JCBS, Vol. 4, Issue 4, 263-268.
- Bahraini, N.H., Devore, M. D., Monteith, L. L., Forster, J. E., Bensen, S., Brenner, L. A. (2013). The role of value importance and success in understanding suicidal ideation among Veterans. JCBS, Vol. 2, Issues 1–2, 31-38.
Miscellaneous Resources
- ACT for Posttraumatic Anger-Related Problems in Living
- Veterans Health Administration ACT Video Series
- ACT for Returning Vets (and others)
- ACT in Context Podcast Episode 10: ACT for Coping with Trauma and PTSD with Robyn Walser
- Veterans Affairs (VA) SIG Resources webpage (Available to ACBS members only)
ACT for Posttraumatic Anger-Related Problems in Living
ACT for Posttraumatic Anger-Related Problems in LivingH.E.A.T. (Honorably Experiencing Anger and Threat) Protocol
H.E.A.T. (Honorably Experiencing Anger and Threat) ProtocolHEAT Presentation at ISTSS
HEAT Presentation at ISTSSLetting Go of 'Righteous Anger with Willingness
Letting Go of 'Righteous Anger with WillingnessACT for Returning Vets (and others)
ACT for Returning Vets (and others)September 8, 2013
This website (http://www.mirecc.va.gov/apps/activities/lifeguard/) presents the five core ACT processes with non-jargon language. The website’s content is based upon a live workshop, named LifeGuard, that has been delivered to returning Veterans, their families, and first-line responders: police officers, firefighters, clergy, college counselors, and employers. The LifeGuard workshop is a one-time, two hour demonstration that uses skits, physical metaphors, and exercises to present the ACT skills. The workshop was evaluated, and positive findings were generated. If you want to know more about the workshop’s findings, you can read the article’s abstract at the following link: http://psycnet.apa.org/journals/pro/42/1/32/
Although the workshop was developed for returning Veterans and their families, it has been delivered to numerous, diverse groups. It has been well-received and anecdotal reports from audience participants suggest that the skills have proven useful -- through a grant a website was created to deliver the material. The LifeGuard workshop and the accompanying web version are educational in nature and are not intended to be a substitute for therapy. The reason for both the workshop and the website is to present ACT skills to the general public, Veterans and non-Veterans alike, so that they can share the skills with one another: peer-to-peer assistance.
Feel free to view the workshop clips and role-play demonstrations on the site and forward the link to whomever you think could benefit from the ACT core processes. The website is free; you do not have to register or identify yourself in any way to log onto the site.
For more information contact Vince Roca
jvroca82@yahoo.com
Other resources on the ACBS Website:
ACT in the US Department of VA
Veterans Health Administration ACT Video Series
Veterans Health Administration ACT Video SeriesVeterans Health Administration ACT Video Series (created by Matthew Boone)
- Defusion: https://www.youtube.com/watch?v=BXAzdXJGMeE
- Acceptance: https://www.youtube.com/watch?v=jrmKtaMqOh4
- Observing Self: https://www.youtube.com/watch?v=kl5cyCXelZc
- Presence: https://www.youtube.com/watch?v=kthk-vmQ02A
- Values & Committed Action: https://www.youtube.com/watch?v=yoVmoOnjscM
- Willingness: https://www.youtube.com/watch?v=qq3u578T1z8
ACT and Islamic Research
ACT and Islamic ResearchACT AND ISLAMIC RESEARCH
This list was initially assembled in February 2022 by Ali Kolahdouzan and Hajar Movahedi Motlagh. There is a deep resonance between ACT and Islam, and there are a myriad of studies on ACT from largely Islamic countries. The list of randomized controlled trials includes literally hundreds of studies from such countries, especially Iran.
This list is of articles or studies that examine ACT ideas in light of Islamic teachings, modify standard ACT elements to fit Islamic culture, suggest how that might be done, or that compare ACT to other conditions that may reflect on such issues. This list is of relevance to the entire ACT community. There are similar efforts in other cultures, language communities, and religous groups, and while the specifics of these modifications may differ, there is much to learn about the strategy for modification across groups.
Journal Articles
Qazanfari, A. (2020). Evaluation and Critique of Modifying Acceptance and Commitment Therapy Therapeutic Approach Based on Quranic Teachings and Hadith. The Journal of Educational Doctrines in Quran and Hadith, 6(1), 125-145. Retrieved From: https://www.magiran.com/paper/2262567
Montazer, A., Nemati, F., Rahimi Nasab, M. H., & Mazidi Sharafabad, A. M. (2016). Enrichment of Acceptance and Commitment Therapy (ACT) using Islamic teachings and Islamic mysticism. Second National Conference on New Studies and Research on Educational and Psychological Sciences in Iran, Qom. COI: CTCONF02_042 Retrieved From: https://civilica.com/doc/677908/
Jamshidian Qaleh Shahi, P., Aghaei, A., & Golparvar, M. (2017). Comparison between the Effect of Positivistic Islamic Approach modified with Persian Cultural Teaching and Acceptance and Commitment Therapy on Psychological Well-Being of Infertile Women in Isfahan. Nursing and Midwifery Journal, Urmia Univeristy of Medical Sciences, Iran, 15(1), 48-57. Retrieved From: https://www.sid.ir/fa/journal/ViewPaper.aspx?ID=286682
Borghei, S. H., Roshan, R., & Bahrami, H. (2018). Effectiveness of a Group Therapy based on Acceptance and Commitment and Spirituality Therapy on Obsessive Beliefs and Quality of Life of People with Obsessive-Compulsive Disorder. The Middle Eastern Journal of Disability Studies, 10(6), 6-16. Retrieved From: http://research.shahed.ac.ir/WSR/WebPages/Report/PaperView.aspx?PaperID=137900
Burghai, Sh., Roshan, R., & Bahrami, H. (2020). Comparison between two group therapies based on a religious spiritual therapy and Acceptance and Commitment Therapy on improving mood and depressive disorder of Women with obsessive-compulsive disorder.. The Journal of Psychology and Religion, 13(1). 39-56. Retrieved From: https://www.noormags.ir/view/fa/articlepage/1612966/
Jahanbakht, M., & Bagheri, F. (2017). Analysis of Acceptance and Commitment Therapy: A Step Toward Normative (Monotheistic) Psychology. The Journal of Educational Science from Islamic Point of View, 5(8), 5-33. COI: JR_EDUC-5-8_001. Retrieved From: https://civilica.com/doc/703893
Khanaliloo, R., & Lotfiekashani, F. (2020). The Effectiveness of Spirituality-Based Acceptance and Commitment Therapy on Depression and Dysfunctional Attitudes in Patients with Multiple Sclerosis. The Journal of Quran and Medicine, 5(1), 93-109. Retrieved From: https://www.sid.ir/fa/Journal/ViewPaper.aspx?ID=577948
Aghili, S.M., & Malek, F. (2021). Comparison between acceptance and commitment therapy and mindfulness-based cognitive therapy on spiritual health and blood pressure of hemodialysis patients in Gorgan. Shenakht Journal of Psychology and Psychiatry, 8 (5), 81-94. Retrieved From: http://shenakht.muk.ac.ir/browse.php?a_code=A-10-1566-9& slc_lang=fa& sid=1
Hassanzadeh, R., Mirzaian, B., Fazeli, M., & Khajvand, A. (2019). Effectiveness of Positivist Psychology Education with the Islamic Approach on Psychological Capital in Cardiovascular Patients. Religion and Health, 7(1), 39-48. Retrieved From: https://www.magiran.com/paper/2029658
Zamani, E., moharrami, R. (2021). Psychological Analysis of Rumo Poetry Based on the Acceptance and Commitment Therapy (ACT) Approach. Research on Mystical Literature (Gowhar-I-Guya), 15(1), 195-214. DOI: 10.22108/jpll.2021.126847.1565 Retrieved From: https://jpll.ui.ac.ir/article_26075.html
Noruzi, A., Moradi, A., Zamani, K., & Hassani, J. (2017). Comparison of the effectiveness of Logotherapy based on Rumi's thought with Acceptance and Commitment Therapy on the psychological well-being of the elderly. The Journal of Research in Psychological Health, 11 (3), 41-61.
DOI: 10.29252/rph.11.3.41 Retrieved From: https://rph.khu.ac.ir/article-1-3021-en.html
Tanhan., A. (2019). Acceptance and Commitment Therapy with Ecological Systems Theory: Addressing Muslim Mental Health Issues and Wellbeing. The Journal of Positive Psychology and Wellbeing, 3(2), 1-23. DOI:10.47602/jpsp.v3i2.172. Retrieved From: https://www.researchgate.net/publication/336107155_Acceptance_and_Commitment_Therapy_with_Ecological_Systems_Theory_Addressing_Muslim_Mental_Health_Issues_and_Wellbeing
Laela, F. N. (2013). Bimbingan dan konseling islam dengan Acceptance and Commitment Therapy (ACT) terhadap seorang ibu yang minder mempunyai anak cact fisik di Desa Tambakromo Kecamatan Cepu. Bimbingan dan Konseling Islam, Dakwah dan Ilmu Komunikasi IAIN Sunan Ampel. Retrieved From: http://catalog.uinsby.ac.id//index.php?p=show_detail& id=81057
Bahattab, M. & AlHadi, A. N. (2021). Acceptance and commitment group therapy among Saudi Muslim females with mental health disorders. The Journal of Contextual Behavioral Science, 19, 86-91. DOI: https://doi.org/10.1016/j.jcbs.2021.01.005 Retrieved From: https://www.sciencedirect.com/science/article/pii/S2212144721000065
Kaplaner, K. (2019). Spirituality in the context of acceptance and commitment therapy (ACT). The Journal of Spiritual Psychology and Counseling, 4, 351–358. DOI: 10.12738/spc.2019.4.3.067 Retrieved From: https://dergipark.org.tr/en/download/article-file/979325#:~:text=In%20the%20process%20of%20ACT,threatening%20diseases%20is%20spiritual%20coping
Shah, N., & Shah, M. (2021). Incorporating Islamic Principles into Therapy with Muslim American Clients. In: Pasha-Zaidi N. (eds) Toward a Positive Psychology of Islam and Muslims. Cross-Cultural Advancements in Positive Psychology, 15. Springer, Cham. DOI: https://doi.org/10.1007/978-3-030-72606-5_11 Retrieved From: https://link.springer.com/chapter/10.1007/978-3-030-72606-5_11
Karekla, M., & Constantinou, M. (2010). Religious coping and cancer: Proposing an acceptance and commitment therapy approach. Cognitive and Behavioral Practice, 17(4), 371–381. DOI:https://doi.org/10.1016/j.cbpra.2009.08.003 Retrieved From: https://psycnet.apa.org/record/2010-07125-001
Kara, E. (2020). Main Strategies of Mindfulness and Acceptance Psychotherapies and Islam. The Journal of Eskiyeni, 40, 377-406. DOI: https://doi.org/10.37697/eskiyeni.672921 Retrieved From: https://dergipark.org.tr/en/pub/eskiyeni/issue/53109/672921
Thesis and Dissertations
Kolahdouzan, S. A., Kajbaf, M. B., Oraizi, H. R., Abedi, M. R., & Mokarian, F. (2020). Development of two death anxiety treatment packages based on the treatment of acceptance and commitment and Abrahamic religions with emphasis on Islam and comparing their impact on mental health and quality of life of cancer patients [Doctoral dissertation, Isfahan University]. Iran Institute of Information Science and Technology Research Repository. https://ganj.irandoc.ac.ir/#/articles/6a9d884fe36706a1cbfd49b24a99f6b0
Movahedi Motlagh, H., Kajbaf, MB., & Fatehizade, M. (2018). A Comparison between of the therapeutic approach based on Acceptance and Commitment Therapy and an Approach that Developes the Islamic Pattern of Acceptance and Commitment Therapy [Master’s thesis, Isfahan University]. The library of the University of Isfahan Research Repository. http://lib.ui.ac.ir/dL/search/default.aspx?Term=16421& Field=0& DTC=
Comparison of the psychological impact of the Acceptance and Commitment Therapy with dhikr in Islamic teachings [Master’s thesis, Tarbiat Modares University].
Iran Institute of Information Science and Technology Research Repository. https://ganj.irandoc.ac.ir/#/articles/8330e2f6eea5164d3fbdaffda1b35916
Mohammadi, A., Mottaghi, S. H., Behjati Ardakani, F., & Kordi, E. (2019). The effectiveness of training based on Acceptance and Commitment Therapy and Islamic teaching on impulsive decision making and the psychological flexibility of addicted Women [Master’s thesis, Ardekan University]. Iran Institute of Information Science and Technology Research Repository. https://ganj.irandoc.ac.ir/#/articles/9f50f6bd624037c1d8be0925d1283dab
Mojahedian, Z., & Dehghan Manshadi, M. (2020). The effectiveness of group therapy based on Acceptance and Commitment Therapy and an Islamic approach to mental health and life expectancy of the elderly in Yazd province [Master’s thesis, Islamic Azad University of Yazd]. Iran Institute of Information Science and Technology Research. Repository.https://ganj.irandoc.ac.ir/#/articles/5820f37baadca3f7a7885321cf05fc1b
Tashakori Bafghi, A., & Zarei Mahmoudabadi, H. (2021).The effectiveness of Acceptance and Commitment Therapy with Islamic approach on existential anxiety of housewives in Bafgh. [Master’s thesis, Islamic Azad University of Yazd].
Iran Institute of Information Science and Technology Research Repository. https://ganj.irandoc.ac.ir/#/articles/686d09bb3a952f3a92c7e0feb6610528
Hakimian, M. M., Sadrposhan, N., & Abolhassani Shahreza, F. (2018). The effectiveness of acceptance and commitment group therapy (ACT) with Islamic approach on diabetes control, increasing self-care behaviors and reducing anxiety and depression in patients with type 2 diabetes in Yazd province[Doctoral dissertation, Yazd University]. Iran Institute of Information Science and Technology Research Repository. https://ganj.irandoc.ac.ir/#/articles/51300387b1d7c0d5859114fa92805b34
Tanhan, A., & Linnenberg, D. (2017). Spiritual Strength: The use of Acceptance and Commitment Therapy (ACT) with Muslim Clients [Master’s thesis, University of North Carolina at Greensboro]. University of North Carolina at Greensboro Research Repository. https://www.researchgate.net/publication/357164226_Spiritual_Strength_The_use_of_Acceptance_and_Commitment_Therapy_ACT_with_Muslim_Clients
Akter, N. (2020). Acceptance and Commitment Therapy Protocol for the Treatment of Substance Abuse Among Muslims [Doctoral dissertation, Widener University]. ProQuest Dissertations Research Repository. https://www.proquest.com/openview/0ec9a5cb5b273a72b952dffa1bc105d0/1?pq-origsite=gscholar& cbl=18750& diss=y
ACT for Law Enforcement
ACT for Law EnforcementThank you for visiting this page dedicated to working with active or retired federal, county, state, municipal, military, or college law enforcement professionals. In providing behavioral health education and training to law enforcement professionals, I use a simple and intuitive tool that I call the "Crosshairs" (Gallo, 2017). It's a diagram adapted from the "ACT Matrix" by Kevin Polk (2011; see also Polk, Schoendorff, Webster, & Fabian, 2016).
The Crosshairs Diagram
Imagine for a moment that you just washed some silverware, and you’re sorting it into a kitchen cabinet drawer. You can put forks, spoons, butter knives, and sharp knives into different piles according to their common characteristics. It turns out that you can do the same thing with situations in life.
The Crosshairs diagram is a highly-effective tool to help you look at situations that show up in your life, divide, and sort the things you do in them. Using the Crosshairs diagram results in being more aware of whether the things you do to deal with painful thoughts, feelings, and situations are helpful or unhelpful in living your values at work, home, or in other important areas of life.
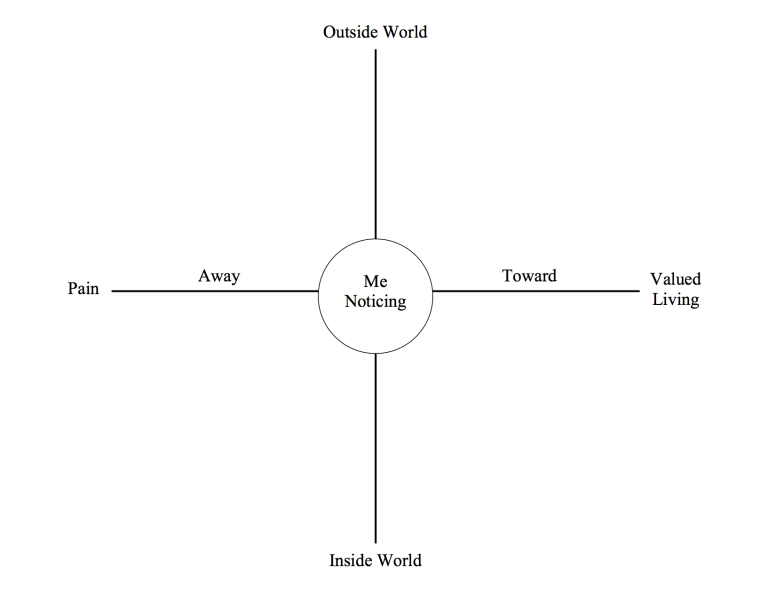
To learn more about the Crosshairs diagram, watch the animated video below. It tells the story of the Crosshairs diagram and its different parts. It helps make the diagram simple to use and puts it all in perspective.
The Blue Life Academy is a free website focused on behavioral health education and training for law enforcement professionals, including
- Acceptance and commitment training
- Breathing, mindfulness, and relaxation training
- Critical incident support information
- Suicide prevention tools
- Resources for military service members
- And more stuff...
The Blue Life Coach app is a FREE behavioral health toolkit designed to help law enforcement professionals lower stress, improve performance during challenging situations, improve sleep, reduce emotional reactivity, increase situational awareness, sharpen mental clarity and problem-solving skills, and live life with more purpose and vitality, guided by their values. The FREE app is available on the Google Play and Apple iTunes stores.
References
- Gallo, F. J. (2017). Bouncing back from trauma: The essential step-by-step guide for police readiness. North Charleston, SC: CreateSpace Independent Publishing Platform.
- Gallo, F. J. (2019). Police use of force. In J. Kitaeff (Ed.), Handbook of police psychology (2nd ed.). New York, NY: Routledge, Psychology Press.
- Polk, K. (2011). Psychological flexibility training (PFT): Flexing your mind along with your muscles. Seattle, WA: Amazon Digital Services.
- Polk, K., Schoendorff, B., Webster, M., & Olaz, F. O. (2016). The essential guide to the ACT Matrix: A step-by-step approach to using the ACT Matrix model in clinical practice. Oakland, CA: Context Press.
How to Contact Me
Frank J. Gallo, Ph.D.
Licensed Psychologist
Retired Law Enforcement
Blue Life Behavioral Health
P.O. Box 8592
Cranston, RI 02920
Phone: (413) 575-8145
Email: support@bluelifeacademy.com
Blue Life Academy: https://bluelifeacademy.com
Blue Life Coach: https://bluelifecoach.com
ACT in Private Practice
ACT in Private PracticeACT in Private Practice Videos
There is a Research in Clinical Practice Collaborative Special Interest Group (SIG) that ACBS members can join. The Research in Clinical Practice Collaborative SIG has resources webpage available to ACBS members.
ACT in Private Practice Resources
ACT in Private Practice ResourcesThere are many resources throughout the ACBS website which could be useful for clinicians seeking to apply ACT in private practice. Below is a list of a few highlights. If you would like to suggest an addition to this list, please log in and make a comment below.
Note: You will need to be logged in as an ACBS member to access these resources.
ACT as a Brief Intervention
In this video, Kirk Strosahl, one of the developers of ACT, discusses the unique challenges faced by practioners who may have only a short amount of time to impact therapeutic change. He provides some clinical tips, as well as demonstrates their application in a role-play:
http://contextualscience.org/act_as_a_brief_intervention_clinical_training_work
ACT in the Treatment of Trauma
In this video, former ACBS President Robyn Walser provides clinical tips for the application of ACT in the treatment of trauma:
http://contextualscience.org/acceptance_and_the_treatment_of_trauma
Acceptance and Commitment Therapy for Insomnia (ACT-I) by Dr Guy Meadows
Acceptance and Commitment Therapy for Insomnia (ACT-I) by Dr Guy MeadowsACT for INSOMNIA (ACT-I) by Dr Guy Meadows (PhD)
Abstract
Acceptance and Commitment Therapy (ACT) offers a unique and gentle non-drug based approach to overcoming chronic insomnia. It seeks to increase people’s willingness to experience the conditioned physiological and psychological discomfort commonly associated with not sleeping.
Such acceptance paradoxically acts to lessen the brains level of nocturnal arousal, thus encouraging a state of rest and sleepiness, rather than struggle and wakefulness. Additional focus on valued driven behaviour also acts to avert unhelpful patterns of experiential avoidance and promote the ideal safe environment from which good quality sleep can emerge. The application and merits for using ACT approaches such as acceptance and willingness, mindfulness and defusion and values and committed action for the treatment of chronic insomnia are discussed and compared to the traditional cognitive behavioural strategies.
Introduction
Sleep involves a slowing of psychological (e.g. decision making, problem solving and emotional readiness) and physiological (e.g. heart rate, breathing rate, blood pressure, bowel movements and muscle tone) processes at the end of the day. It is a natural act that can’t be controlled and is characterized by an acceptance of the natural rise in sleep drive associated with nighttime and a willingness to let go of wakefulness.
By contrast, chronic insomnia is a difficulty sleeping that is characterized by a state of hyper arousal, which interferes with the natural ability to initiate or maintain sleep or achieve restorative sleep. Where insomnia is the primary disorder, the initial trigger is often resolved. But sleeplessness is maintained by a vicious cycle whereby poor sleep initiates worry about not sleeping, which in turn elevates arousal levels leading to further poor sleep. The adoption of unhelpful coping strategies and the movement away from valued living act to create an inflexible relationship with sleep.
Cognitive behaviour therapy for insomnia (CBT-I) is the most widely used treatment method. Its primary focus is based around symptom reduction via changing the cognitive and behavioral conditions that perpetuate the insomnia. It most commonly achieves this through a series of 1-hour interventions delivered over a 6 – 8 week period.
Whilst these interventions have been proven to be effective at reducing insomnia rates, some patients still struggle. Complaints typically focus around the non-workable nature of the process used and the continued need for patients to diarize their sleep and thoughts throughout the intervention. Dalrymple et al. (2010) investigated how incorporating principles from Acceptance and Commitment Therapy (ACT; Hayes et al. 1999) into the treatment of insomnia could potentially enhance the adherence to and acceptability of such traditional CBT-I approaches. This opens up the debate as to whether ACT approaches alone could be an effective insomnia treatment. The rationale for using ACT approaches within the treatment of insomnia and the practical ways in which it could be implemented into therapy sessions are discussed in this poster.
Acceptance
The vicious cycle of insomnia demonstrates that it is the unwillingness of patients to experience the unwanted thoughts, emotions and physical sensations associated with not sleeping and the ensuing struggle with them that heightens arousal levels and perpetuates sleeplessness. Most insomniacs can provide a long list of control-based strategies, including traditional CBT-I techniques, they have implemented and yet which have failed to improve their sleep. This focus on symptom reduction, which if ineffective simply perpetuates the vicious cycle. It could be more effective to teach patients to adopt a more accepting attitude towards what spontaneously arises when experiencing difficulty sleeping. The greater willingness to experience poor sleep results in fewer struggles, less arousal and paradoxically greater levels of sleepiness.
Practically, any initial insomnia assessment should include a detailed review of the failed techniques previously used to improve sleep. Lundh (2005) suggests that such an awareness of the futility of control-based strategies could then be used as a starting point from which to guide a patient towards alternative acceptance based approaches.
Mindfulness:
Mindfulness is the ability to objectively and non judgmentally take notice of your internal and external experiences as they unfold. It can help insomniacs to stand back and observe their level of wakefulness or unwanted thoughts and emotional reactions without becoming overly entangled or judging them, a quality that is inherent in the normal act of falling to sleep. Shifting patients towards an attitude of acceptance rather than the CBT-I focus on symptom reduction seen with many of the traditional relaxation strategies could be a way of short-circuiting the vicious cycle of insomnia.
Practically, insomniacs can be taught to mindfully notice their senses and the movement of their breath, which they can then practice during the day. At night such exercises can be used to help patients to notice and let go of their struggles and return back to the present moment (e.g. noticing the touch of the duvet on their toes or the gentle movement of their breathe). Care must be taken to highlight the potential risk and futility of using mindfulness as a tool to control the level of relaxation or sleep and to confirm the benefits of objective noticing (e.g. the use of the quicksand metaphor can be helpful at this point).
Defusion
Defusion describes the ability to see thoughts and emotions for what they are (e.g. naturally occurring cognitive and emotional responses) and create space for them to exist, rather than fusing with them or seeing them as something that needs to be removed, before sleep can be restored.
Such acceptance once again bypasses the need to struggle with such internal content by changing the patient’s relationship with the content. It could be argued that such an energy efficient and low arousal approach is more nocturnally intuitive than the traditional CBT-I based cognitive restructuring, which requires patients to challenge their thoughts and then create new alternative and balanced ones in their place.
Practically, patients spend time identifying their unwanted thoughts, emotions, physical sensations and urges that show up when they don’t sleep. They are then taught basic defusion exercises such as objectively describing, naming and welcoming unhelpful thoughts when they arrive in the night such as “I am having the thought that…” or “Hello, ‘coping’, ‘medication’ and ‘ill health’ thoughts”. For emotions and physical sensations, patients can practice ‘Physicalizing’ exercises such as objectively locating and describing them and imagining them as objects and giving them a physical shape and colour.
Valued Sleep Actions
A normal sleeper has a strong relationship with their bed and bedroom, meaning they can fall to sleep or return back to sleep very quickly and with little effort. In contrast, an insomniac has a negative sleep association meaning they become cognitively and emotionally alert at the point of trying to sleep (e.g. conditioned bedtime arousal). The adoption of unhelpful coping strategies in order to control sleep (e.g. going to bed early, sleeping in the spare room or sleeping during the day), not only perpetuates poor sleep, but also results in a reduction in valued living (e.g. not being able to go out at night, share a bed with a partner or schedule early appointments), something that patients cite as one of the main reasons for struggling with sleep in the first place.
CBT-I approaches the problem by asking patients to follow a series of strict rules known as Stimulus Control Therapy (SCT), see table 1. The aim is to limit the time patients spend in the negative state or engaging in non-sleep activities, in the hope of developing a positive association, whereby sleep onset occurs rapidly on getting into bed. Whilst SCT is widely used, many patients complain that its strict nature is counter intuitive and goes against normal valued sleep actions, see table 1. The result is that anxiety and arousal levels associated with the bedroom and sleep are unhelpfully heightened.
In contrast, teaching patients to commit to making behavioural changes in line with their sleep and life values, whilst being willing to experience the unwanted elements of the negative association could be an effective way of re-establishing a positive association between sleep and bed. The aim is that by promoting a healthy and flexible approach to sleep, any negative associations and therefore arousal levels would be reduced, creating a platform from which natural sleep could emerge effortlessly.
Table 1. Valued Sleep Actions
Allow normal bedroom activities
CBT-I: NO - Use the bed for sleep and sex only
ACT-I: YES - Allow calm non sleep activities such as reading in bed
Go to bed when either tired or sleepy
CBT-I: NO - Only when sleepy
ACT-I: YES - Both states allowed
Stay in bed, if awake at night
CBT-I: NO - If not asleep within 15mins, go to a spare room/read
ACT-I: YES - Focus on resting and welcoming discomfort
Allow daytime naps
CBT-I: NO - Avoid all daytime napping
ACT-I: YES - Allow a short (<20mins) daytime naps
Restricting Sleep
Sleep is regulated by an internal body clock and a sleep homeostat, to keep it on time and create its cyclical drive. A normal sleeper keeps a fairly regular pattern by going to bed and getting up at roughly the same time four days per week and a little later on the weekend. A common coping strategy of many insomniacs is to change their sleep wake cycle in the hope of getting a little more sleep (e.g. going to bed earlier, lying in later or catching up during the day). Whilst such action may make cognitive sense, they do in fact worsen nocturnal sleep by lowering the sleep efficiency (SE), the percentage of time spent in bed asleep.
CBT-I approaches this problem using Sleep Restriction Therapy (SRT), which restricts the time in bed to actual sleeping time only so as sleep drive increases, so will sleep consolidation, which can then be steadily titrated back to a normal level. Whilst such an approach can be affective, some patients struggle with the concept of spending less time in bed. Many insomniacs also present with sleep anxiety and so any suggestion of restricting the amount of time in bed is often met with increased levels of anxiety and alertness, thus counteracting any of the positive benefits of an increase in sleep drive, possibly explaining the low adherence rates.
Practically, it is therefore advised that patient anxiety levels be considered before the implementation of sleep restriction. If anxiety levels are found to be high, then treatment should be focused on increasing patient willingness to experience the anxiety, before then considering sleep restriction at a later date (e.g. assuming reduced anxiety levels did not lead to improved sleep).
Conclusions
This poster puts forward the rationale for using Acceptance and Commitment Therapy for Insomnia (ACT-I) and its potential benefits over traditional cognitive behavioural treatments. It suggests that acceptance and mindfulness based approaches are intuitively, psychologically and physiologically more in tune with the natural process of deactivation associated with falling to sleep. It places importance on the act of adopting valued sleep actions, whilst being willing to experience the heightened cognitive and emotional processes that present in response to not sleeping. Ultimately it seeks to promote a high level of sleep flexibility, thus leading to less struggle and arousal, improved sleep quality and energy conservation and enhanced quality of life.
References
Dalrymple, K.L., Fiorentino, L., Politi, M.C., & Posner, D., (2010). Incorporating Principles from Aceptance and Commitment Therapy for Insomnia: A Case Example. J Contemp Psychother, 40: 209-217.
Hayes, S.C., Strosahl, K.D., & Wilson, K.G. (1999). Acceptance and commitment t: An experiential approach to behaviour change. New York: Guilford Press.
Lundh, L.G., (2005). The Role of Acceptance and Mindfulness in the Treatment of Insomnia. J of Cog Psychother, 19: 29-39.
Additional Information
Dr Guy Meadows (PhD) is a sleep physiologist who runs The Sleep School a private sleep clinic in London focusing on the use of Acceptance and Commitment Therapy in the treatment of Insomnia. For further information please visit: www.thesleepschool.org or email: guy@thesleepschool.org.
Alternatively please follow FB: The Sleep School or Twitter: DrGuyMeadows
Or see his ACT-I book: The Sleep Book
Acceptance and commitment Therapy for Sport
Acceptance and commitment Therapy for SportACT for Sport
Helping Athletes Create Psychological Flexibility
by Stephen Renwick, MSc, BSc & ACT Therapist
After you are finished watching the video, click here for an episode of the Sport Psychology Podcast
Bible resources for Christian clients
Bible resources for Christian clientsOver the past few years, as I have learned more and more about ACT, I have been adding to spreadsheets I started some time back. I initially named the lists after the six ACT processes. It seems that there has been some interest in these lists and therefore I am attaching them here. I tried for some time to do this in a format that could be added to, but it seems that this is not possible. So suffice it to say that I do not by any means consider these lists to be exhaustive of the topics at hand. They have merely grown from my own personal study, and my own experience of the processes. I moved on to using these with clients and in workshops. So far they have been well received, to the best of my knowledge. It would be very useful to receive comments and additions to the lists.
Updated to add:
There is also a manual available for working with Christian clients at www.actwithfaithbook.com as well as a Special Interest Group for working with Christian clients..
Workplace/Coaching
Workplace/CoachingThere are Special Interest Groups (SIGs) that ACBS members can join:
- Acceptance and Mindfulness at Work: Applying Acceptance and Commitment Therapy And Relational Frame Theory to Organizational Behavior Management
- Acceptance and Commitment Coaching (Coaching Distinctive Features)
- Maximize Your Coaching Effectiveness with Acceptance and Commitment Therapy
- The Mindful and Effective Employee: An Acceptance and Commitment Therapy Training Manual for Improving Well-Being and Performance
- Prosocial: Using Evolutionary Science to Build Productive, Equitable, and Collaborative Groups
- The psychology of enhancing human performance: The Mindfulness-Acceptance-Commitment (MAC) approach
Journal of Contextual Behavioral Science
- Puolakanaho, A. Tolvanen, A. Kinnunen, S.M., Lappalainen, R. (2020) A psychological flexibility -based intervention for Burnout:A randomized controlled trial. Journal of Contextual Behavioral Science, 15, 52-67.
- Puolakanaho, A., Tolvanen, A., Kinnunen, S.M., Lappalainen, R. (2018) Burnout-related ill-being at work: Associations between mindfulness and acceptance skills, worksite factors, and experienced well-being in life. Journal of Contextual Behavioral Science, 10, 92-102.
- Veage, S., Ciarrochi, J., Deane, F. P., Andresen, R., Oades, L. G., & Crowe, T. P. (2014) Value congruence, importance and success and in the workplace: Links with well-being and burnout amongst mental health practitioners. Journal of Contextual Behavioral Science, 3, 258-264.
Books
BooksCOVID-19 Therapy Resources
COVID-19 Therapy ResourcesWe've gathered therapy resources for COVID-19, also known as Coronavirus. These resources (as well as the comments) have all been submitted by ACBS members.
Resources for the public, as well as resources in other languages, are included here.
Resources for Helping Children:
Resources designed for use with children, adolescents, and teenagers are included here.
A list of resources for therapists, including Teletherapy resources, are included here.
Looking for a Therapist?: This page lists members of ACBS who have identified themselves as ACT therapists and who are available for online/teletherapy and consultation. You can use the search feature to look for therapists by country, province/state, or city.
Are you an ACBS member therapist who provides Video/Teletherapy for clients? Click here to let us know. (ACBS staff will then update your online listing)
Are you looking for Video/Teletherapy software options? We have provided a few suggestions here.
The ACTing with Technology SIG has put together a page highlighting a few recommendations and guidelines for online/video therapy here.
Resources for Helping Children
Resources for Helping ChildrenBelow are therapy resources for COVID-19, also known as Coronavirus. These resources (as well as the comments) have been submitted by ACBS members.
• Child Mind Institute - has helpful articles and resources.
• Coping with stress - tip sheet for parents.
• Coronacast - a podcast by an Australian physician.
• Coronavirus visual story - for young and less literal children.
• Dave the Dog - A Nurse Dotty book.
• Health Care Toolbox - has some resources for children
• Healthy Habits Childrens Activity Book - activities for younger children.
• Helping Children Cope with Stress
• Just For Kids: A Comic Exploring The New Coronavirus
• Mind Heart - A resource requiring less literacy.
• Play School in Australia segment.
• Stay Here ebooklet - a tool for parents to help their family cope with being at home during COVID-19, and manage the stress, uncertainty and changes of not being able to attend school, work and social/leisure activities. It is based on ACT and compassion-based approaches.
The New Pandemic Pioneers - booklet and worksheets
Resources Available in Other Languages:
• My Hero is You (developed via a global survey of children aged 4-10 years) - includes translations to UN languages.
• mhpss.net - toolkit has many resources and languages archived there. They also have resources used previously for similar infectious disease outbreaks here.
• Parenting advice - from UNICEF and others.
• Turkish resources for covid parenting.
Looking for a Therapist?: This page lists members of ACBS who have identified themselves as ACT therapists and who are available for online/teletherapy and consultation. You can use the search feature to look for therapists by country, province/state, or city.
DO YOU HAVE ADDITIONS TO THIS LIST? Please login to your member account and "comment" below to add your suggestions and we'll continue to incorporate them into this page.
Resources for Therapists
Resources for Therapists• ABA Telehealth for Families - explains more about the process of virtual treatment and the importance of it.
• ACT Malaysia team resources - an informal group of ACT practitioners from Malaysia under the name "ACTMalaysia" compiled a small number of COVID-19 related resources, including some translational work.
• APA webinar “Telepsychology Best Practice 101 - currently available free of charge.
• Coping after a long stay in the hospital - Informational pamphlet.
• COVID-19 Resources Page - from the Association of Psychologists in Academic Health Centers (APAHC).
• COVID-19 Resource Documents - from Jason Washburn at Northwestern University.
• Doing What Matters In Times of Stress - free illustrated ACT self-help book released by WHO.
• From helpless to hero: Promoting values-based behavior and positive family interaction in the midst of Covid-19 - an article published in Behavior Analysis in Practice (authored by: Tom Szabo, Sarah Richling, Dennis Embry, Tony Biglan, and Kelly Wilson)
• Grief and Bereavement Resources - A conversation with Dr. Katherine Shear of Columbia University's Center for Complicated Grief at the Columbia School of Social Work and a handout with advice and resources related to managing bereavement around COVID-19.
• Malaysian
• Moderators of social Isolation and mental health outcomes during COVID-19 - a webinar presented by Brooke Smith and one of her students on moderators of social isolation and mental health outcomes during COVID-19. It presents the findings from their paper that was recently published in JCBS, in which we found that psychological inflexibility and intolerance of uncertainty moderated the relationship between social isolation and depression, anxiety, stress, and well-being. A link to the paper is here.
• POTC Episode # 164: Pandemic Stress: Strategies from Acceptance and Commitment Therapy with Debbie and Diana - The Psychologists Off the Clock podcast recently posted and episode on pandemic stress and ACT. We hope it helps spread the word on the utility of psychological flexibility during these challenging times. Take a listen and share with your clients, family and friends!
• Prosocial workshop for working with groups in the context of COVID-19 - Corinna Stewart and Beate Ebert would like to share a workshop they did on Prosocial in the context of COVID-19. The link leads to a raw version of the video, which has yet to be edited. We have listed the times for each section below:
0:5:24: Video introduction to Prosocial during the Ebola epidemic in Sierra Leone
0:13:32: Introduction to the workshop in Mandarin
0:17:21: Overview and background
0:26:56: Example of Prosocial use in Sierra Leone
0:31:40: CBS and Prosocial, Narratives about prosociality - Media and COVID-19 reporting
0:43:44: The Prosocial Process: The ACT Matrix; Interactive Individual (0:55:00) and group (1:05:45) Matrices
1:17:40: Overview of 8 core design principles
1:32:00: Q&A session with participants
• Telehealth training for Mental Health Professionals (through PESI) - What are the legal and ethical risks? Is distance therapy even effective? How do I get started? For a limited time, you can get this online training for free - Click the link, add the online training to your cart and use code TELEFREE at checkout.
• The Mental Health & Psychosocial Support Network - This is an international collaboration of mental health and psychosocial support that has been running for many years. It’s a portal with resources for crisis or disasters — 3600 members. They share protocols and resources and network together when a disaster or crisis is occurring anywhere in the world. Well worth joining if you happen to need quick info. There are already a number of coronavirus resources up there — for a variety of circumstances.
• Resource for presenting the Matrix to clients online - Laura Crosby from the UK and Benji Schoendorff recorded a Zoom meeting which demonstrates how Zoom can be used to present the matrix to clients. Here is a link to the video on their YouTube channel. It doubles as a zoom for clinical practice tutorial displaying some of its versatile tools and options. (Requires the link as it is not a public video on their YouTube channel.)
o In addition to Zoom, there is a PowerPoint presentation and the matrix cards. Here is a link to a cloud where you’ll find the PowerPoint presentation for you to use and/or adapt.
o The cloud also contains screenshots that can be made with Zoom when you do a Matrix with clients and a pdf of the matrix cards in English for you to use with clients.
• Notification of Enforcement Discretion for Telehealth Remote Communications During the COVID-19 Nationwide Public Health Emergency - from the U.S. Department of Health & Human Services.
• Values-based Illustration for COVID-19 (Italian version included here)
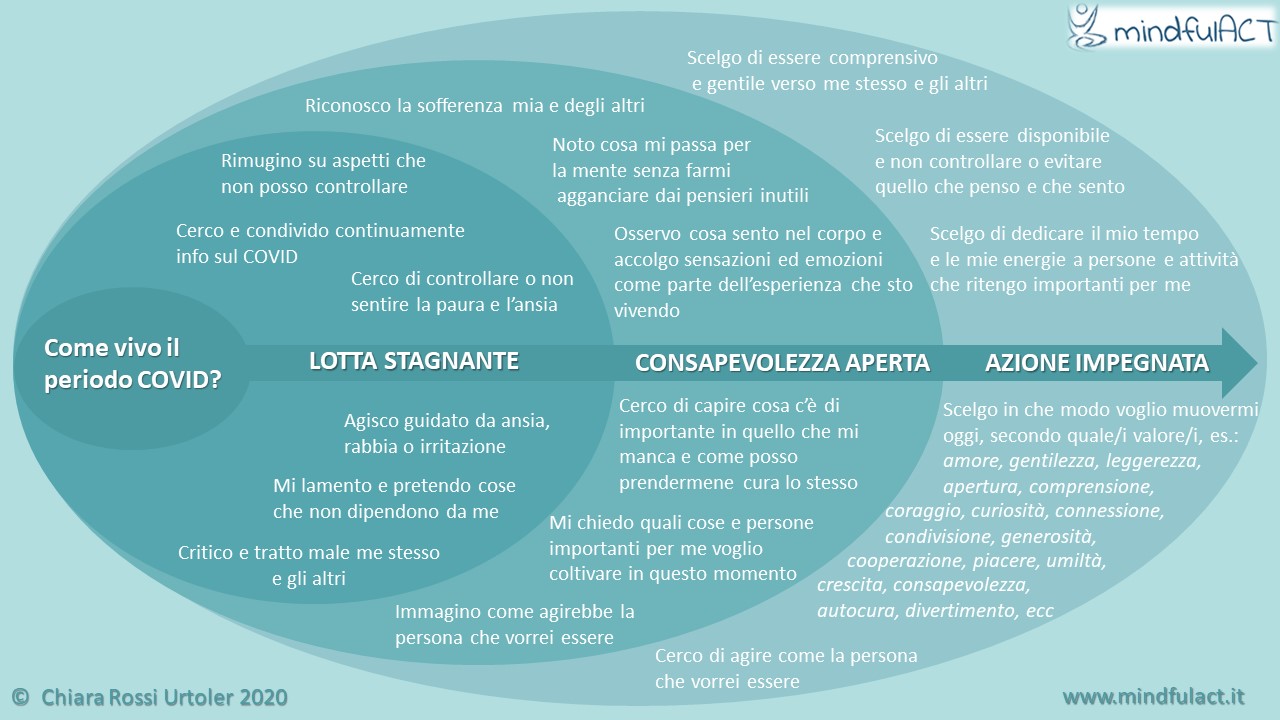{kind=link}
• Video therapy and other technology resources - The ACTing with Technology SIG has a few useful resouces pages, including some recommendations on video therapy.
Looking for a Therapist?: This page lists members of ACBS who have identified themselves as ACT therapists and who are available for online/teletherapy and consultation. You can use the search feature to look for therapists by country, province/state, or city.
Are you an ACBS member therapist who provides Video/Teletherapy for clients? Click here to let us know. (ACBS staff will then update your online listing)
Are you looking for Video/Teletherapy software options? We have provided a few suggestions here.
DO YOU HAVE ADDITIONS TO THIS LIST? Please login to your member account and "comment" below to add your suggestions and we'll continue to incorporate them into this page.
Resources for the Public
Resources for the PublicBelow are some therapy resources for COVID-19, also known as Coronavirus. These resources (as well as the comments) have been submitted by ACBS members.
• ACT and anxiety for organisations - Yesterday for the first time a client asked me (Robb Archer) to write something for their 200k (!) employees about ACT per se. They wanted something about anxiety and this is what I pulled together.
• ACT Companion: The Happiness Trap App - available free of charge for the next few months. Just download the app from the Apple app store or Google Play store and then enter the code TOGETHER on the subscription page to unlock all the app content for three months. The code is valid until the end of June. Please feel free to share this code with all your colleagues, clients, friends, family or anyone you think would benefit. NB: Unfortunately the app is not compatible with the latest version of Android, so may not be supported on some newer Android devices.
• ACT and Cornavirus prevention blog post (Brazilian Portugese)
• ACT Mindfully products - completely free of charge for the next few months.
o Mindfulness Skills Vol 1 - these are ‘ACT classics’ - e.g. leaves on a stream, mindful breathing
o Mindfulness Skills Vol 2 - more challenging exercises - e.g. long body scan, pure awareness
o The Reality Slap – Exercises & Meditations Self-compassion, loving-kindness and mindful grounding exercises
• ACT Video Series and Exercises on Coping with COVID-19 - a video series and exercises on how the six core processes of ACT apply to coping with COVID-19. It is geared especially to those who are on the front lines.
• An Acceptance And Commitment Therapy Approach To Coping With COVID-19 For Healthcare Workers - A podcast with Joe Tatta and Julie Hamilton.
• Checking In With Susan David (a podcast) - ACT-consistent resource that may be helpful to your clients: a podcast developed with TED on how to deal with tough emotions during this pandemic.
o Loneliness in the era of COVID - Susan just released a dialogue Steve Hayes had with her on loneliness in the era of COVID.
• Coping with Coronavirus-Related Anxiety: Free Webinar - lots of ACT-related advice shared in a free webinar on how to deal with coronavirus-related anxiety and other challenges. Jonathan Kaplan, Anne Marie Albano, Dean McKay, and Rebecca Sachs discuss the following:
o Coping with uncertainty and anxiety
o Continuing to live a purposeful and meaningful life
o Practicing proactive resilience to counter potential feelings of sadness, depression, and helpless
o Balancing “being on vacation” and maintaining structure/ and consistency in parenting
o Maintaining social contact and strengthening relationships with the people you’re living with (even in small spaces)!
• "Coping with Crisis" - Free app with psychological tools to help support you in these times of crisis. We have created three themes that all have a mini-course with three lessons (with option to do in small video-sharing groups), exercises and meditations. It is available for anyone for free. Feel free to use yourself, recommend to clients or friends if you find useful.
• COVID & ACT video - a short video for the public about staying mentally healthy during the COVID-19 pandemic, and includes the 6 ACT processes.
• Covid Coach - a mobile app designed to help people stay sane, connected, and cope with stress, navigate parenting and care-taking, find resources during the COVID-19 pandemic. Covid Coach is free, secure, evidence-in formed, federally-funded by US intended for everyone and developed by staff at National Center for PTSD. You'll find the Apple version here. The Android version is available here.
•COVID Resources for Fire Service Members - Zachary Isoma shared mindfulness exercises specific for fire service members called Internal Situational Awareness Training (iSAT). He created a quick tips and resources guide for dealing with COVID stress as a firefighter. Feel free to download, print, and distribute. He also attached a free resource guide on dealing with stress provided by Joe LaCognata at Fire Rescue Support, who offers chaplaincy with fire rescue.
• Digital Resources from Italy – We have developed material, audio files for meditation, and list of resilient actions. All this material is available to you (in Italian, but you can easily google-translate it and adapt).
o Spanish Translation of these resources available below
• FACE COVID pamphlet - all about using ACT to deal with the crisis. Please feel free to share it with anyone and everyone who might benefit (Illustrated eBook version, Infographic version, Instagram Version (pdf), Text only version, and YouTube animation of FACE COVID)
{kind=link}
o Go here for translations in 20 plus languages
• Facing Pandemic Fears with an Awake Heart - Tara Brach provides a talk (audio or video), which is in response to the current health crisis. The included meditation, based upon her RAIN (mindfulness + compassion) approach, is quite nurturing.
• Free mindfulness & meditation resources - Here is a curated and annotated list of FREE resources to help us live easily and meaningfully, even as we’re confined to our homes. As you might expect from us at the SoHo CBT + Mindfulness Center, most of these resources focus on mindfulness and meditation.
• Guided mindfulness practice, plus Q and A with Jon Kabat-Zinn - If you can't join the live sessions you can watch the recorded videos at your leisure. There are two ways to join: by zoom or facebook.
• Heroes in Your Home - Lay version of the article written by Sarah Richling, Dennis Embry, Tony Biglan, Kelly Wilson, and Tom Szabo.
• Hope This Helps Video - A short video (by Joanne Steinwachs) for ED staff.
• How can ACT help prevent coronavirus? - A Brazilian behavior-analytic blog (in Portugese), with some links between WHO recommendations for prevention highlighted by ACT processes as a mean to establish some EO's to adhere to the recommendations. Hope it helps.
• How Can We Cooperate When the Pandemic Is Driving Us Apart? - Paul Atkins, coauthor of Prosocial, explains what will help us work together in the face of disaster.
• Pasos Prácticos Para Responder de Manera Eficaz a las Consecuencias Psicológicas del Confinamiento (Practical Steps for Responding Effectively to the Psychological Consequences of Confinement) - this guide (in Spanish) has been developed by Dr. Carlos Salgado, based on functional contextualism, about "attention based on what is important for the person-ACIP." Here is an interactive infographic that he has created, related to the attached document.
• Pencil and Screen - This is a resource for essential workers who are struggling to support their school aged students while still showing up in their communities to keep people safe and supplied.
• Presentations on Anxiety (and more) - This links to presentations on anxiety, depression, gratitude, chronic illness, grief/loss, relationships, stress management, etc., and, a brief mindfulness meditation. Here is the worksheet that accompanies the first of 6 presentations on anxiety. Worksheets that accompany the other presentations can be found at www.easeap.com.
• Seven Ways to Stay Calm and Avoid Anxiety
• Steering Through The Storm: Self-Help eBook - Turkish Resources for Psychological Challenges Triggered by the COVID-19 Outbreak.
• Suicide Prevention Lifeline (U.S. based) - Lifeline Chat connects individuals with counselors for emotional support and other services via web chat. Lifeline Chat is available 24/7 across the U.S.
• Taking Care of Your Mental Health During the COVID-19 Pandemic - this is 3 min animated video. Please distribute freely as you see fit.
• TED Connects: Community and Hope-How To Be Your Best Self Self In Times of Crisis - It’s available on video here, and as a podcast on TED Talks Daily here.
• The Marginal Gains Handbook – Practical ideas to survive and thrive in the age of Coronavirus.
• The Ordinary Corona Hero: You - How you can act heroically in the face of a pandemic.
• Turkish Resources For Healthcare Professionals - Recommendations (in Turkish) for Healthcare Professionals in the Pandemic Process and Steering Through The Storm: Self-help Video Series (in Turkish).
• Virtual Meditation for Asian, Pacific Islander, DESI Americans (APIDA)
• Virtual resources for those recovering from addiction and related issues -
o In the Rooms - A free global online recovery tool that offers 130 weekly online meetings for those recovering from addiction and related issues.
o Online Meetings directory for Alchoholics Anonymous
o SMART Recovery - Self-Management And Recovery Training (SMART) is a global community of mutual-support groups. Mutual support meetings are free and open to anyone seeking science-based, self-empowered addiction recovery.
Looking for a Therapist?: This page lists members of ACBS who have identified themselves as ACT therapists and who are available for online/teletherapy and consultation. You can use the search feature to look for therapists by country, province/state, or city.
DO YOU HAVE ADDITIONS TO THIS LIST? Please login to your member account and "comment" below to add your suggestions and we'll continue to incorporate them into this page.
ACT for Anxiety related to COVID-19
ACT for Anxiety related to COVID-19Translations of the FACE COVID Pamphlet
Translations of the FACE COVID PamphletThe FACE COVID pamphlet is about using ACT to deal with the crisis. Please feel free to share it with anyone and everyone who might benefit.
Thank-you to everyone who has taken the time to send us their translations.
o Arabic Version (thanks Dr Gaceb Boualem and Dr Hassan Boudassamout)
o Danish Version (thanks Johannes A Drescher Joergensen)
o Dutch Version (thank you John Morawski)
o French Version (thanks Lise Loury)
o German Version (thanks Threo Schelp)
o Greek Version (thanks Maria Karekla)
o Hebrew Version (thanks Lilac Friedman)
o Italian Version (thank you Salvatore Torregrossa)
o Japanese translation of the Text only version (thanks Manabu Yoshimoto)
o Japanese translation of the Illustrated eBook version (thanks Horiba Erika)
o Lithuanian Version (thanks Vilma Jazgeviciute)
o Malay Version (thanks Eugene Koh)
o Norwegian Version (thanks Kristin Evjen)
o Polish Version (thanks Agnieszka Wroczyńska)
o Portuguese Version one (thanks Graça Areias)
o Portuguese Version two (thanks Bruno Carraça and C. Magalhães)
o Portuguese Version (Brazilian - thanks Priscila Rolim de Moura)
o Romanian Version and Romanian Video (thanks Ioana Pascaru)
o Russian Version (thanks Ilya Rozov)
o Serbian Version (thanks Darko Tomic and Natasha Lazareski)
o Simplified Mandarin (thanks Eugene Koh)
o Spanish Version of the Infographic (thank you Hugo Ceballos)
o Spanish Version one (thank you Carlos Irurzun)
o Spanish Version two (thanks Enrique Parada)
o Swedish Version (thanks Nicklas Lasko)
o Traditional Chinese (thanks Anthony Tong and the ACBS Hong Kong Chapter)
o Turkish Translations (thanks Seher Cömertoğlu & Fatih Yavuz) - (Illustrated eBook version, Infographic version, and YouTube animation of FACE COVID)
o Vietnamese Version (thanks Gia Hoang)
Training
TrainingVisit the Training section for additional resources.
See the webpage Resources for Learning More About ACT for a comprehensive list of resources.
Peer Consultation
Peer ConsultationAnother great way to create resources and support is to form a Peer Consultation Group.
They are not hard to form. Just click here for advice on how to do so and for a list of peer consultation groups.
Several ACBS Chapters and Affiliates have peer consultation groups.
Read the Journal of Contextual Behavioral Science article Creating a peer-led acceptance and commitment therapy consultation group: The Portland model (JCBS, Volume 4, Issue 3, July 2015)
Training DVDs
Training DVDs-
Introduction to ACT, Steven C. Hayes: Psychotherapy Networker Audio Home Study Course A318
This is a six hour, clinician-friendly audio course on ACT. You can get it as a CD. Good introduction to the model. A bit pricey and the audio is not always great during questions, but you get CEUs.
-
Hayes, S. C. (Ed.). (2007). ACT in Action DVD series. Oakland, CA: New Harbinger.
A set of six DVDs on the following topics: Facing the struggle; Control and acceptance; Cognitive defusion; Mindfulness, self, and contact with the present moment; Values and action; and Psychological flexibility. The tapes include several ACT therapists from around the world in addition to Steve, including Ann Bailey-Ciarrochi, JoAnne Dahl, Rainer Sonntag, Kirk Strosahl, Robyn Walser, Rikard Wicksell, and Kelly Wilson. As the marketing folks say: you've read the books, now see the movies.
- Acceptance and Commitment Therapy with Steven C. Hayes. Part of the Systems of Psychotherapy APA Psychotherapy Video Series.
-
A 100 minute video published by the APA of Steven Hayes conducting ACT with an actual client. Shows several aspects of the model in a single session, including some that are characteristic and distinct from other approaches. Good for training.
- A 90 minute ACT tape from the 2000 World Congress of Behavioral and Cognitive Therapy is available from ABCT. It shows Steve Hayes working with a client (role-played by a graduate student—Steve did not, however, meet the “client” or know their “problem” before the role playing started so it appears relatively realistic). Some sound problems but good for training.
- ABCT has a taped interview with Steve Hayes about the development of ACT and RFT as part of their “Archives” series. Steve thinks this means he is old.
-
Eifert, G. (2004). Tutorial: Acceptance-Based Behavior Therapy for Anxiety Disorders (DVD).
The Association for Behavior Analysis has a one hour DVD of a short talk by Georg Eifert on ACT for Anxiety Disorders. It doesn’t really show you at all how to do ACT, but does give a nice introduction to how ACT can be used for Anxiety.
-
Barnes-Holmes, D. (2006). Tutorial: Relational Frame Theory (DVD).
This is a DVD of a tutorial given by Dermot Barnes-Holmes at the Association for Behavior Analysis conference. The presentation focuses on the main concepts of RFT and how they are currently being used to develop conceptual and empirical analyses of areas such as symbolic meaning, analogical reasoning, rule-governance, and implicit attitudes.
-
Roche, B. (2006). Tutorial: Making the World A Better Place...Context by Context and Frame by Frame (DVD).
This is a DVD of a tutorial given by Bryan Roche at the Association for Behavior Analysis conference. The tutorial includes an outline of RFT and functional contextualism as well as a discussion of the application of RFT to a range of social issues.
Materials for Presenting ACT and Teaching Resources
Materials for Presenting ACT and Teaching Resources CommunityMaterials for Presenting ACT
Materials for Presenting ACTThis is the old parent page (<2011) for presentations (e.g., Powerpoint Slides), individual slides or figures, handouts, or related materials for sharing ACT with others.
ACT 2-day Training
ACT 2-day TrainingPresented by Steve Hayes in Boston.
ACT Colloquium
ACT ColloquiumACT Gone Wild
ACT Gone WildACT Oceania II - The History of ACT and RFT
ACT Oceania II - The History of ACT and RFTACT Oceania II--ACT with Depression
ACT Oceania II--ACT with DepressionACT State of the Evidence (2008)
ACT State of the Evidence (2008)Originally presented by Steve Hayes at ACT SI 2; Philadelphia, PA, USA 2005. Updated July 2008.
ACT for Anxiety- Kenneth Cole
ACT for Anxiety- Kenneth ColeACT for Anxiety-Gary Powell
ACT for Anxiety-Gary PowellACT for Chronic Pain
ACT for Chronic PainACT for Male Sexual Problems
ACT for Male Sexual ProblemsACT for PTSD
ACT for PTSDACT materials - Dr Kingsley Mudd
ACT materials - Dr Kingsley MuddSome useful client education tools and handouts from my ACT presentations.
Cheers
Dr Kingsley Mudd MBBS BMedSci FRACGP
Townsville, Qld, Australia
Email - kjkmudd@bigpond.net.au
ACT with Couples
ACT with CouplesThis is a presentation called:
The Application of Acceptance and Commitment Therapy to Couples in Distress
Presented by Casey Capps and Ragnar Storaasli
May 30th, 2006
ABA Atlanta
Powerpoint presentation attached below.
ACT with Depression
ACT with DepressionACT with Parents and Families
ACT with Parents and FamiliesACT:Model and Application
ACT:Model and ApplicationAnxiety and Forgiveness
Anxiety and ForgivenessThe two attachments below are to introductory ACT-based presentations on Forgiveness and Anxiety that I gave to staff and students at the UK school where I work.
Please feel free to use/amend/distribute them for non-commercial purposes. Thanks to the ACT artists and conceptualisers of the illustrations used therein.
Downloadable files below.
Gary
ContextaFlex: Connecting FC, RFT and the Hexaflex
ContextaFlex: Connecting FC, RFT and the HexaflexA PowerPoint presentation to show beginners the importance of the underlying philosophy (functional contextualism) and theory (RFT) behind the practice of ACT.
Presented by: Jerold Hambright, Ph.D., Kevin Polk, Ph.D., John Agee, Ph.D. Veterans Affairs Hospital, Togus, Maine, USA
Drugs and Alcohol Action Teams ACT 2 day training course
Drugs and Alcohol Action Teams ACT 2 day training coursePowerpoint from 2 day training courses I have run for Drugs and Alcohol Action Teams (DAATS). The course is usually run after a two day CBT training.
AIMS OF INTRODUCTION TO ACT TWO DAY WORKSHOP
In this workshop, you will learn:
The position of ACT in relation to other cognitive behavioural therapies
The six core principles of ACT, and how to adapt them to different clinical populations
Become aware of tools to develop and strengthen psychological acceptance
Become aware of ways to rapidly reduce the believability of negative thoughts (without challenging them)
Develop an understanding of mindfulness, and how to use ACT therapeutically
How to innovate your own mindfulness techniques
How to utilise ACT in a variety of clinical problems
How to use interventions based on metaphor, paradox and experiential exercises
How to apply ACT in your own life, to create a sense of vitality, meaning and fulfilment
How to use ACT to help you cope with the stresses of difficult clients
How to access and experience a transcendent sense of self
How to fundamentally change your relationship with unwanted thoughts and feelings
How to help clients connect with their core values, and take committed action
Teaching methods will be a mixture of didactic and experiential learning. Handouts for future use will be provided.
COURSE TUTOR
Nadim I. Siddiqui
Associate Fellow British Psychological Society, BA (Hons) Psychology, MSc (Cognitive Behavioural Psychotherapy), Cert. REBT, Cert. Stress Man., Dip. Couns., EMDR level 2. Psychologist, Cognitive Behavioural Psychotherapist, EMDR Practitioner
From Mechanism to Functionalism - or: What is Avoided in Emotional Avoidance?
From Mechanism to Functionalism - or: What is Avoided in Emotional Avoidance?Handouts from Introductory and Advanced ACT Workshops by Russ Harris
Handouts from Introductory and Advanced ACT Workshops by Russ HarrisRuss Harris (from Australia) responded to a query about handouts that could be shared with the ACT community by volunteering a couple handouts that he uses in his workshops (see below). After looking at them, I find them to be a very valuable and practical aid for ACT therapists. If you want to talk to him about them, his contact info is described in the handouts.
Update by Russ Harris on April 22, 2008:
Thanks for posting my worksheets up, Jason. I regularly update them, and I'll send some them to you as I do so. Just a note: the extracts from 'The Happiness Trap' in these handouts are from the Australian version. It has been significantly rewritten for the USA version. If you don't already know about it, 'The Happiness Trap' is unique amongst ACT books in that it is the only one that has been written for EVERYONE - therapists, coaches, housewives and astronauts, regardless of whether or not they have ‘mental health issues’ - which also explains ACT in a simple, easy-to-understand manner, without any technical language, or a battery of worksheets and inventories. You can find out more at http://www.thehappinesstrap.com. It is increasingly used as a resource by both therapists and coaches - not only to use with their clients, but also as a way of learning the theory and techniques of ACT in a simple, clear and entertaining manner. (And its ultra-low cost also helps: only $10.50 via www.amazon.com)
Intro to ACT by Guarna and Kubik, Portland, ME June 5, 2009
Intro to ACT by Guarna and Kubik, Portland, ME June 5, 2009Intro to ACT, 2/04/11, Maine Medical Center, Portland -- by Joel Guarna
Intro to ACT, 2/04/11, Maine Medical Center, Portland -- by Joel GuarnaMy powerpoint presentation for this workshop can be found in my blog at this page. You will need to be logged-in to see and download the attachments. If you need it sent to you directly, please email me at joel@whitepinepsych.com
Intro to ACT_Portland, Maine_Guarna_&_Kubik
Intro to ACT_Portland, Maine_Guarna_&_KubikIntroduction to ACT by Joel Guarna, Dover, NH: 3/21/09
Introduction to ACT by Joel Guarna, Dover, NH: 3/21/09Introduction to ACT- Charles Morse
Introduction to ACT- Charles MorseIntroduction to ACT-Julian McNally
Introduction to ACT-Julian McNallyIntroduction to ACT_Boston Consortium_ 2005_Joel Guarna
Introduction to ACT_Boston Consortium_ 2005_Joel GuarnaIntroduction to the Hexaflex
Introduction to the HexaflexTrans-Diagnostic Approach to Problems in Living
Trans-Diagnostic Approach to Problems in LivingWhat is This Thing Called ACT
What is This Thing Called ACTA Presentation at the University of Maryland (College Park) Counseling Center
10/26/2011
Ron Kimball, PhD, CGP, FACFE
What is this Acceptance and Commitment Therapy?
What is this Acceptance and Commitment Therapy?Tips on how to add content to this section
Tips on how to add content to this sectionTeaching Resources
Teaching ResourcesPlease feel free to post any materials (powerpoints, handouts, reading lists, etc) you use to teach your courses including (and beyond) material relevant to:
- ACT
- RFT
- Behaviorism
- Behavior analysis
- Functional contextualism
- History of psychology/clinical psychology, etc
- Philosophy of science
- Third wave
- CBT
- Mindfulness
- Anything else of interest that has shaped you and you share with your students
Abnormal Psychology Text Recommendation
Abnormal Psychology Text RecommendationRonald Comer's Abnormal book has a nice section on ACT.
David Gillanders: Intros to both ACT and RFT
David Gillanders: Intros to both ACT and RFTThis page includes two powerpoints: An introduction to ACT and and introduction to RFT.
Joel Guarna's Introductory materials
Joel Guarna's Introductory materials- Most recent 3-hour workshop at Maine Medical Center, Portland, Maine (2011) posted in my blog.
- Full-day workshops in Portland, Maine and Dover, NH (both 2009).
- Half-day workshop at the Boston Consortium in Clinical Psychology (2005).
- Miscellaneous other ACT presentations (various presenters).
John Forsyth: ACT class Syllabus
John Forsyth: ACT class SyllabusThe Spring 2011 syllabus is below.
Miscellaneous Presentations
Miscellaneous Presentations Joel GuarnaWhat is the Cost of Training in ACT?
What is the Cost of Training in ACT?Because my name is associated with ACT as its instigator and co-developer I often get emails containing questions like this:
My answer usually looks something like this:
If you were diligent you could become competent in ACT in most of the existing ways it is specifically applied just by joining ACBS (contextualscience.org) and systematically availing yourself of the resources there -- hundreds of protocols, tapes, videos, tools etc arraying in a vast "Wiki-stype" site ... especially if you then reached out to local ACBS members and plugging into local meetings and peer supervision groups
The cost to join ACBS is low. We have "values-based dues" meaning we ask people to pay what they think it is worth, based on their ability to pay. There is a $15 minimum (as of 2023) -- and a chunk of that goes to Elsevier for the association journal -- but that minimum itself can be waived if you are too poor to pay it.
Conversely if you want to access paid workshops (etc) they are plentiful and range in price in the usual way. Our annual conventions almost have myriad workshops for free after the initial convention registration, and the price is what is typical for conferences that also include a free lunch.
Bottom line: we live a bit outside of the box your question envisions for us.
There is instead a scientific and professional community focused on a knowledge development and dissemination strategy called "contextual behavioral science." You can learning it all for free if you work hard at it ... and hopefully you can then also contribute your own voice to that development strategy.
- S
Steven C. Hayes
Videoconferencing/ Telehealth software options for therapists
Videoconferencing/ Telehealth software options for therapists
On this page you can find known video/teleconferencing options that might work for you as a mental health professional. These have been submitted by ACBS members.
The ACTing with Technology SIG has put together a page highlighting a few recommendations and guidelines for online/video therapy as well.
(Looking for a therapist in your area who does video/teletherapy? Look here!)
If you have more suggestions, please login to your ACBS account and add a “comment” at the bottom of this page, and we’ll incorporate your suggestion into this page.
Please check each system to verify that any system you choose conforms with any necessary security and privacy requirements in your Country/Province/State as needed. ACBS endorses no particular system, or its privacy statements.
Doxy.me
Doxy.me is easy to use, doesn’t require downloading the program from the client and is free for one-to-one sessions. In the paid version you can have group sessions, share your monitor, and other features.
Zoom
Zoom is also good for individual and group sessions. If you need to facilitate group sessions or need extra options, Zooms paid plans can be more affordable compared to doxy.me. (Zoom has free and paid versions. Secure and non-secure versions.)
Some ideas to Protect against malicious Zoombombing.
G Suite
https://cloud.google.com/security/compliance/hipaa
https://support.google.com/a/answer/3407054?hl=en
JITSI
Jitsi is a free and open source, fully encrypted video conferencing solution that you can use all day, every day, for free - with no account needed. You can also download it for free and run it internally at an organisation not only for staff but for customers and partners too.
To get going just use any room name to create a VC space and invite others to use it.
Some of its features are:
* Auto-view the active speaker or click on any attendee to see their video
* Android and iOS apps
* Text chatting (web only)
* Lock a room with a password
* and more....
THERAPlatform
THERAPlatform is an all in one practice management system. The video portion features ability to use an interactive whiteboard, view videos, share documents and write progress notes during video sessions (as well as in-person sessions). It's secure and HIPAA-compliant. I have no affiliation with THERAplatform and am currently trying it out. On trial, it had better connectivity than experienced with other HiPAA-compliant video systems.
Whereby
https://whereby.com/ easy to use - no extra downloads. (privacy compliance unknown)
Getting Started with Telemental Health - Free 30 minute video
Getting Started with Telemental Health - Free 30 minute videoHello all,
I recently completed a recording for the Association for Behavioral and Cognitive Therapies (ABCT) called "Getting Started with Telemental Health." It's about 30 minutes and provides a quick overview of the basics in providing mental healthcare via tele. The slides have links to find more in depth information as needed. I hope it helps ease some of the difficulties in transitioning to this modality right now.
ABCT Website link (video and slides):
http://www.abct.org/Resources/index.cfm?m=mResources&fa=Telehealth_Kate_Morrison
YouTube link (video only):
All my best,
Kate
--
Kate L. Morrison, Ph.D.
Some more options
Some more optionsAdopted from https://opensource.com/alternatives
Wire
Developed by the audio engineers who created Skype, Wire features secure screen sharing, file sharing, and group chat, administrator management, and the ability to switch between accounts and profiles (work and personal, for example) at will from within the app.
Wire is open source under the GPL 3.0 license and is free to use if you compile it from source on your own server. A paid option is available starting at $5 per user per month (with large enterprise plans also available).
https://wire.com/en/
Jami
Audio and video calls are made through the Jami app, available for GNU/Linux, Windows, and MacOS desktops and Android and iOS mobile devices. You can communicate using either a unique user ID (which the Jami app randomly generates the first time it's launched) or over SIP. You can use your ID and SIP in parallel, switching between protocols as needed, but you must register your ID on the blockchain before it can be used to make or receive communications.
https://jami.net/
Riot
is not just a video-conferencing solution—it's team-management software with integrated group video/voice chat communications. Communication (including voice and video conferencing, file sharing, notifications, and project reminders) happens in dedicated "rooms" that can be organized by topic, team, event, etc. Anything shared in a room is persistently stored with access governed by that room's confidentially settings. A cool feature is that you can use Riot to communicate with people using other collaboration tools—including IRC, Slack, Twitter, SMS, and Gitter.
You can use Riot in your browser (Chrome and Firefox) or via its apps for MacOS, Windows, and Linux desktops and iOS and Android devices. In terms of infrastructure, Riot can be installed on your server, or you can run it on Riot's servers. It is based on the Matrix React SDK, so all files and data transferred over Riot are secured with Matrix's end-to-end encryption.
https://about.riot.im/
Signal
For mobile devices running Android or iOS, the open source Signal app offers end-to-end encrypted voice, video, text, and photos, and it's been endorsed by security and cryptography experts including Edward Snowden and Bruce Schneier and the Electronic Frontier Foundation. Registration is simple: you're identified by your phone number, so all you have to do to register is to use the app. There's a desktop client available, but only for text chat, so it's clear that Whisper Systems, the nonprofit that maintains Signal, intends for this to be a mobile application. It's a perfect marriage between the two clients: you can use the desktop client as you work for brief messages and questions, and pick up your mobile (as you do) when you need to do a quick voice or video consultation.
https://signal.org/
Linphone
is a VoIP (voice over internet protocol) communications service that operates over the session initiation protocol (SIP). This means you need a SIP number to use the service and Linphone limits you to contacting only other SIP numbers—not cellphones or landlines. It's easy to get a SIP number—many internet service providers include them with regular service and Linphone also offers a free SIP service you can use.
With Linphone, you can make audio and HD video calls, do web conferencing, communicate with instant messenger, and share files and photos, but there are no other screen-sharing nor collaboration features. It's available for Linux, Windows, macOS desktops, and Android and iOS mobiles.
http://www.linphone.org/
Nextcloud
provides you with you own private cloud space with plenty of tools geared toward collaboration. After installing Nextcloud on a server, or opening a hosted account, you can add users who can log in and use the Nextcloud interface as a shared workspace. Users can store and share documents and files using either the web interface, or just by dropping them into a Nextcloud directory on their desktop, which gets synchronized automatically with the Nextcloud desktop client. The web interface also features a chat application called Talk, which features the ability to make voice and video calls.
Nextcloud is a shared work space, so once it's installed and configured for your organization, it can probably be the primary virtual office space for your team. It doesn't necessarily have every tool your team needs, but it's an ideal space to share and manage the data your team works on, and to coordinate remote work.
https://nextcloud.com/